
Santiago Reimondez, Álvaro Alcaraz, Santiago Josseau Olguin, Franco José Signorini, Agustina Vigilante, Enzo Giordano, Lucio Ricardo Obeide
Hospital Privado Universitario de Córdoba. Instituto Universitario de Ciencias Biomédicas de Córdoba. Córdoba, Argentina.
Acta Gastroenterol Latinoam 2019;49(1):77-80
Recibido: 21/11/2017 / Aprobado: 02/07/2018 / Publicado en www.actagastro.org el 18/03/2019

Summary
Cystic degeneration of the spleen is a rare entity. True cysts represent 10% of these lesions and the association with CA 19-9 elevation is infrequent. Surgical resection is indicated for cysts greater than 4 cm in diameter. We present two cases of this pathology. The first one was an 18-year-old woman with incidental finding of splenic cyst. CT scan reported a 15 cm diameter upper pole lesion with displacement of adjacent organs, with liquid content and no signs of acute complication. CA 19.9 level was 499 U/ml. Test for hydatidosis was negative. The second patient was a 16-year-old man who complained about pain and palpable tumor in the left hypochondrium. CT scan showed splenic cyst lesion of 20 cm in a similar location. CA 19-9 level was 108 U/ml. Total laparoscopic splenectomy was performed in both cases, without complications. The histopathology showed squamous cystic wall lining compatible with epidermoid cyst. Laboratory control at 3 months reported normalization of CA 19-9 level. Epidermoid cyst is a rare splenic lesion. Total laparoscopic splenectomy in tumors greater than 10 cm and in contact with the splenic hilum has good outcomes in experienced surgeon hands and should be considered the election treatment.
Key words. Splenic cyst, laparoscopic, CA 19-9, splenectomy.
Quiste esplénico benigno gigante: reporte de dos casos con resolución laparoscópica
Resumen
La degeneración quística del bazo es una entidad rara y poco frecuente. Los quistes verdaderos representan el 10% de estas lesiones y su asociación con la elevación del marcador CA 19-9 es poco frecuente. La resección quirúrgica está indicada en tumores mayores de 4 cm de diámetro. Presentamos dos casos de esta patología. El primero fue una mujer de 18 años con hallazgo incidental de quiste esplénico. La TC informó lesión de 15 cm en el polo superior con desplazamientos de órganos adyacentes, de contenido líquido y sin signos de complicaciones agudas. CA 19-9: 499 U/ml. Test para hidatidosis negativos. El segundo caso fue un varón de 16 años con dolor y masa palpable en hipocondrio izquierdo. TC informo lesión quística esplénica de 20 cm con localización similar. CA 19-9: 108 U/ml. En ambos casos se realizó esplenectomía total laparoscópica, sin complicaciones. La histopatología informó epitelio escamoso de recubrimiento sobre una pared quística compatible con quiste epidermoide. El laboratorio de control a los 3 meses mostró normalización del marcador CA 19-9. El quiste esplénico epidermoide es una entidad poco frecuente. La esplenectomía total laparoscópica en tumores mayores de 10 cm y/o en contacto con el hilio esplénico presenta buenos resultados en manos de cirujanos con experiencia y debe ser considerada el tratamiento de elección.
Palabras claves. Quiste esplénico, CA 19-9, laparoscopía, esplenectomía.
Cystic degeneration of the spleen is a rare entity. They are currently classified as parasitic cysts (mainly produced by granulosus echinococcus infection) and non-parasitic cysts. The latter are subclassified as primary or true cysts and secondary or pseudocysts, by the presence of an epithelial or mesothelial lining in the cystic wall.1-3
Epithelial splenic cysts (true cysts) represent approximately 10% of the splenic cystic lesions, usually diagnosed in women under 40 years old.4 The association of this type of splenic cyst with elevation of serum CA 19-9 antigen had been reported.5, 6
Surgical resection is indicated in tumors larger than 4 cm (even in the absence of symptomatology) and with elevation of antigenic markers due to the risk of malignization. Multiple case reports support the laparoscopic approach.5, 7
We present two cases of giant epithelial splenic cysts with serum CA 19-9 antigen elevation, resolved with total splenectomy under laparoscopic approach.
Clinical case 1
An 18-year-old woman was admitted due to car accident, with no medical or surgical history of relevance, she presented multiple excoriations in left shoulder and left quadrants of the abdomen. Labs and x rays were normal.
She was discharged with close follow up. Two days later referred non-specific abdominal pain. Abdominal CT scan was performed, with an incidental finding of a splenic cystic lesion of approximately 15 cm diameter in the upper pole and hilium region, with displacement of adjacent structures (Figure 1-A). No signs of bleeding, infection, septication, or calcification inside the lesion were reported. Serum CA 19-9 was 499 ml/dl. Indirect immunofluorescence assay for hydatidosis was negative.
True splenic cyst was suspected and total laparoscopic splenectomy was proposed. The patient was placed in right lateral decubitus at 45° with left arm extended and in abduction. Two 10-mm trocars and two 5-mm trocars were placed in the left hypochondrium. Exploration of the abdominal cavity showed no signs of liver or peritoneal metastasis.
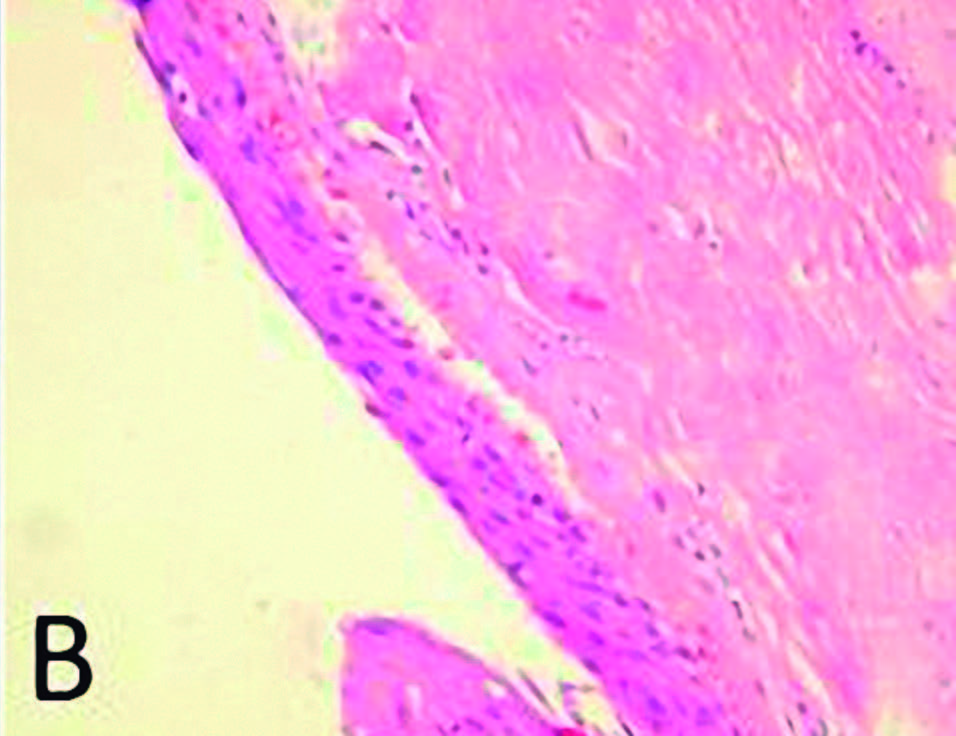
A giant splenic tumor was noticed in the upper pole, without adjacent structures involvement (Figure 1-B). Section of gastrocolic ligament and short vessels was performed with Ligasure® and monopolar coagulation was used for a complete release of splenic angle. After identification and dissection of the pancreas tail, individualization and section of the splenic vessels was done with vascular 45mm stapler. Finally, the diaphragmatic ligament was sectioned and the surgical sample was placed in plastic bag to be removed by Pfannenstiel incision with indemnity of cystic lesion. The histopathology showed cystic tumor of 15 x 12 x 3 cm, with dense connective tissue as a wall covered by squamous epithelium, compatible with true splenic cyst (Figure 2). Laboratory control at three months reported normalization of CA 19-9 level.
Figure 1. A. CT axial view. In upper poles of spleen a Cystic lesion of 15 cm with displacement of adjacent organs.
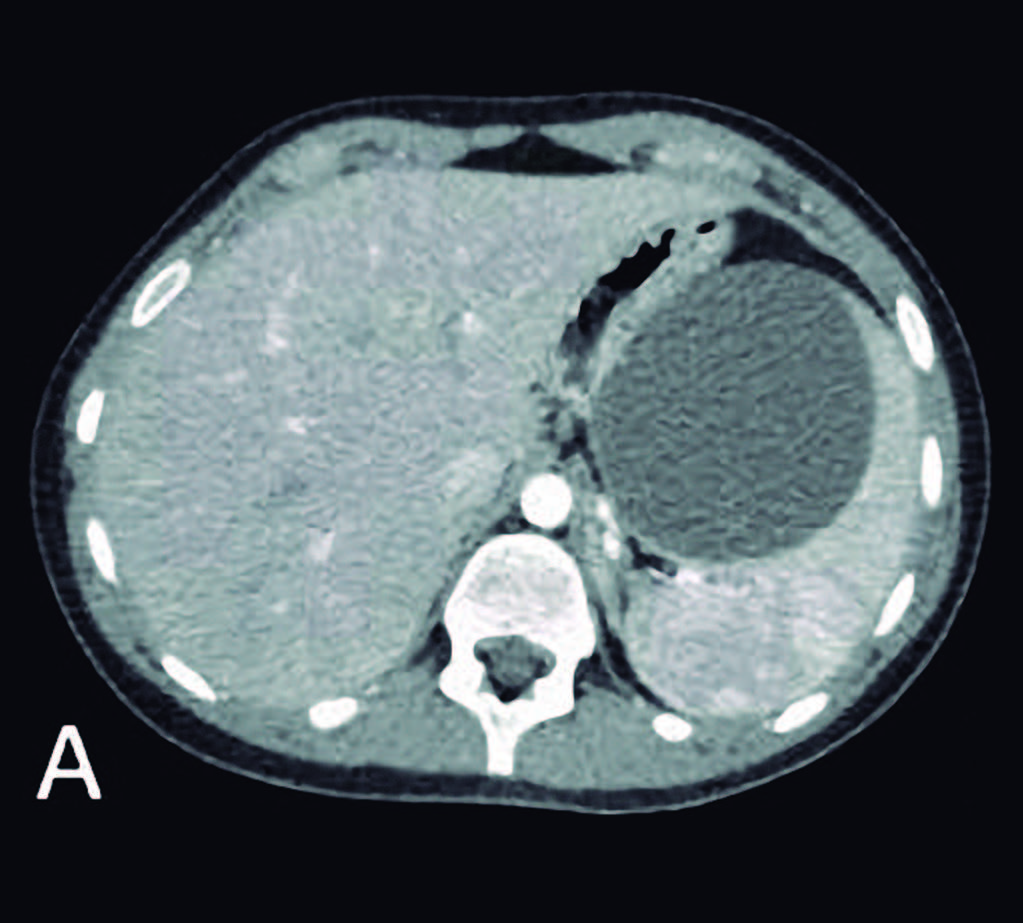
Figure 1. B. Laparoscopic vision of the lesion.
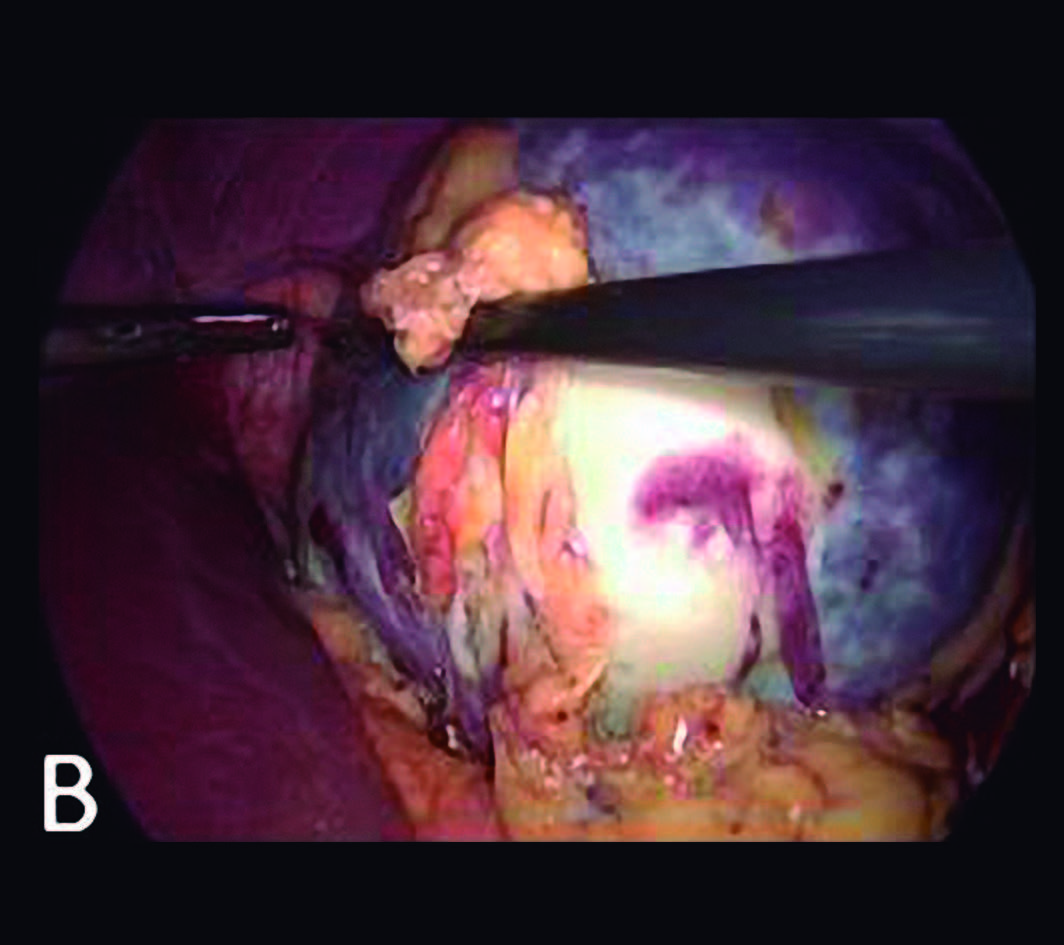
Figure 2. A. Complete surgical sample after drainage of liquid content.
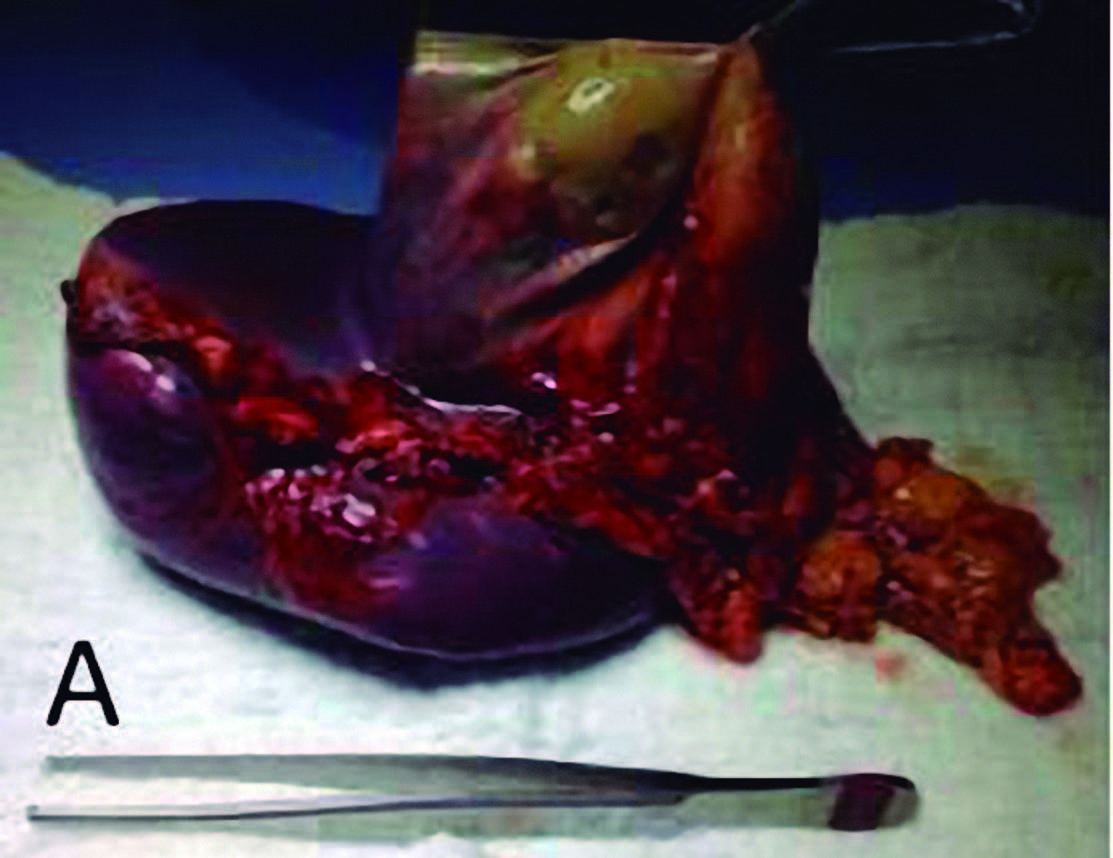
Figure 2. B. Microscopic vision with squamous epithelium of cystic wall lining.
Clinical case 2
A 16 years-old man was admitted complaining about pain and palpable tumor in the left hypocondrium. No medical or surgical history of relevance was recorded. Laboratory and x-rays were normal. Serum CA 19.9 level was 108 U / ml. Immunofluorescence Assay for hydatidosis was reported negative. Abdominal CT scan showed a 20 cm in diameter cystic lesion in the upper pole of the spleen, in contact with the splenic hilum and displacement of adjacent organs (Figure 3). The same proposal was considered.
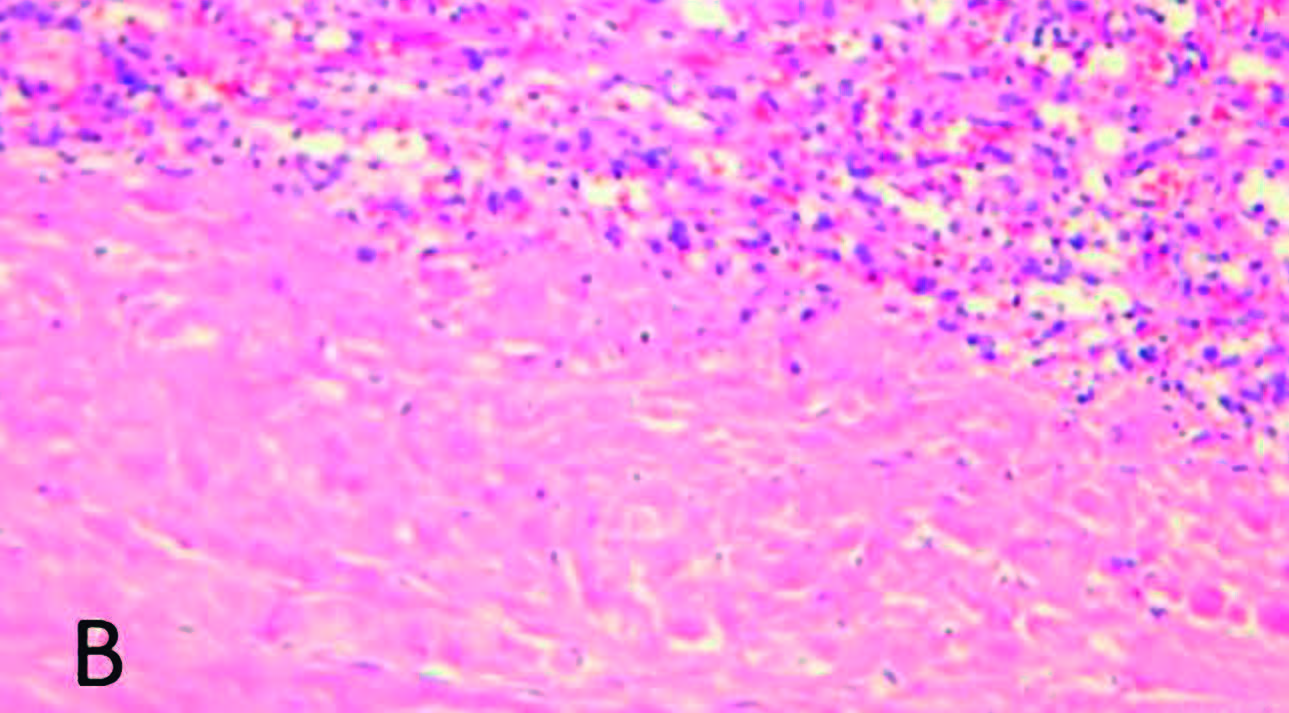
Total laparoscopic splenectomy was performed with the same technique previously described. The histopathological examination revealed a 20 x 11 x 10 cm true splenic cyst with the same epithelium characteristics on microscopic examination (Figure 4). Laboratory control at three months showed normalization of the tumor marker level.
Figure 3. A. CT axial view. B. CT coronal view. Cystic lesion of 20 cm in upper pole of the spleen with displacement of adjacent organs.
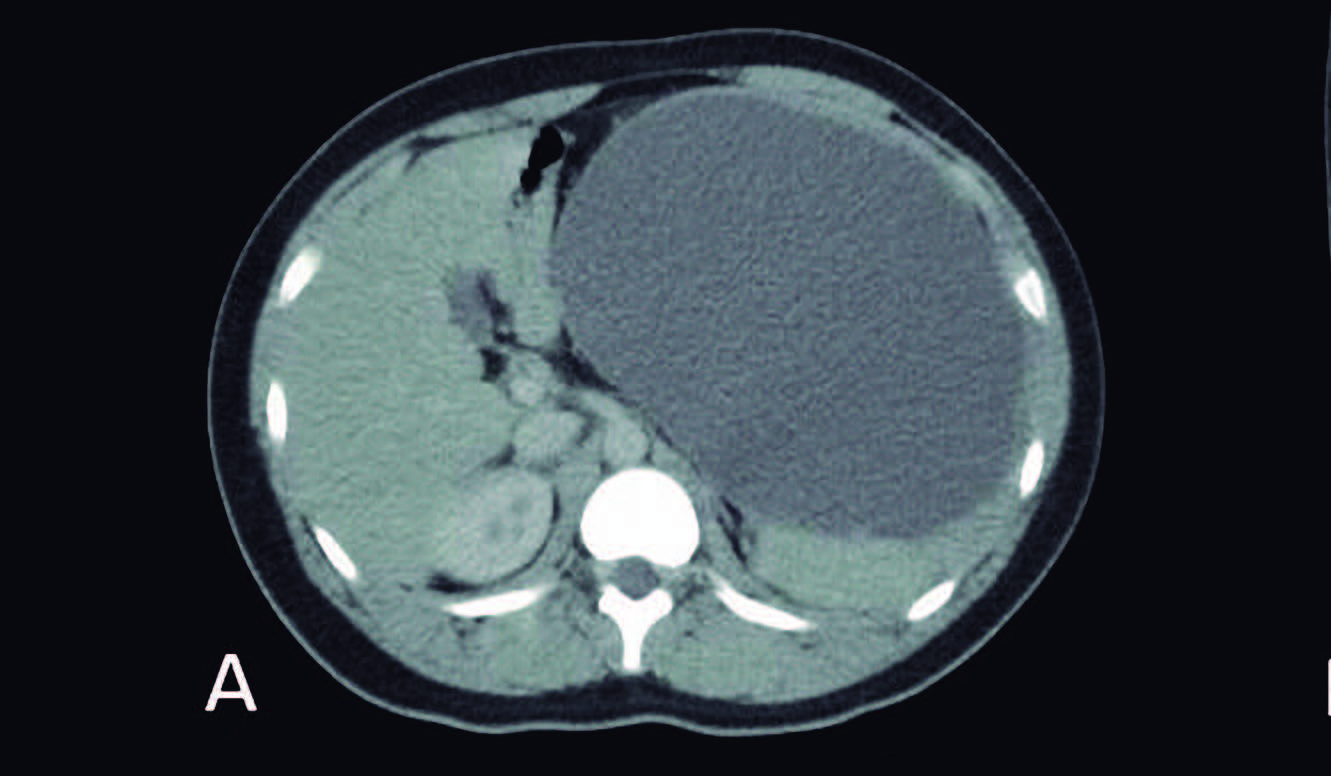
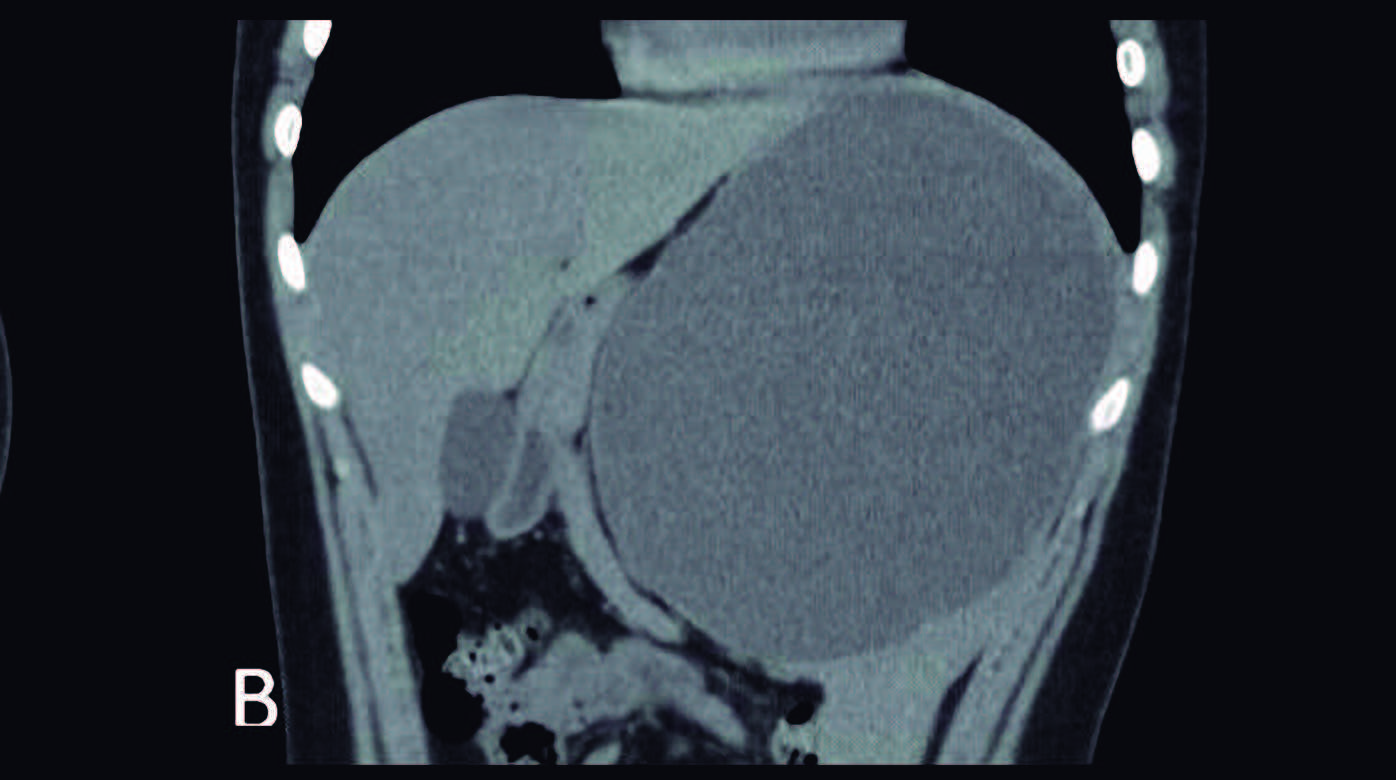
Figure 4. A. Surgical sample after drainage of the content.
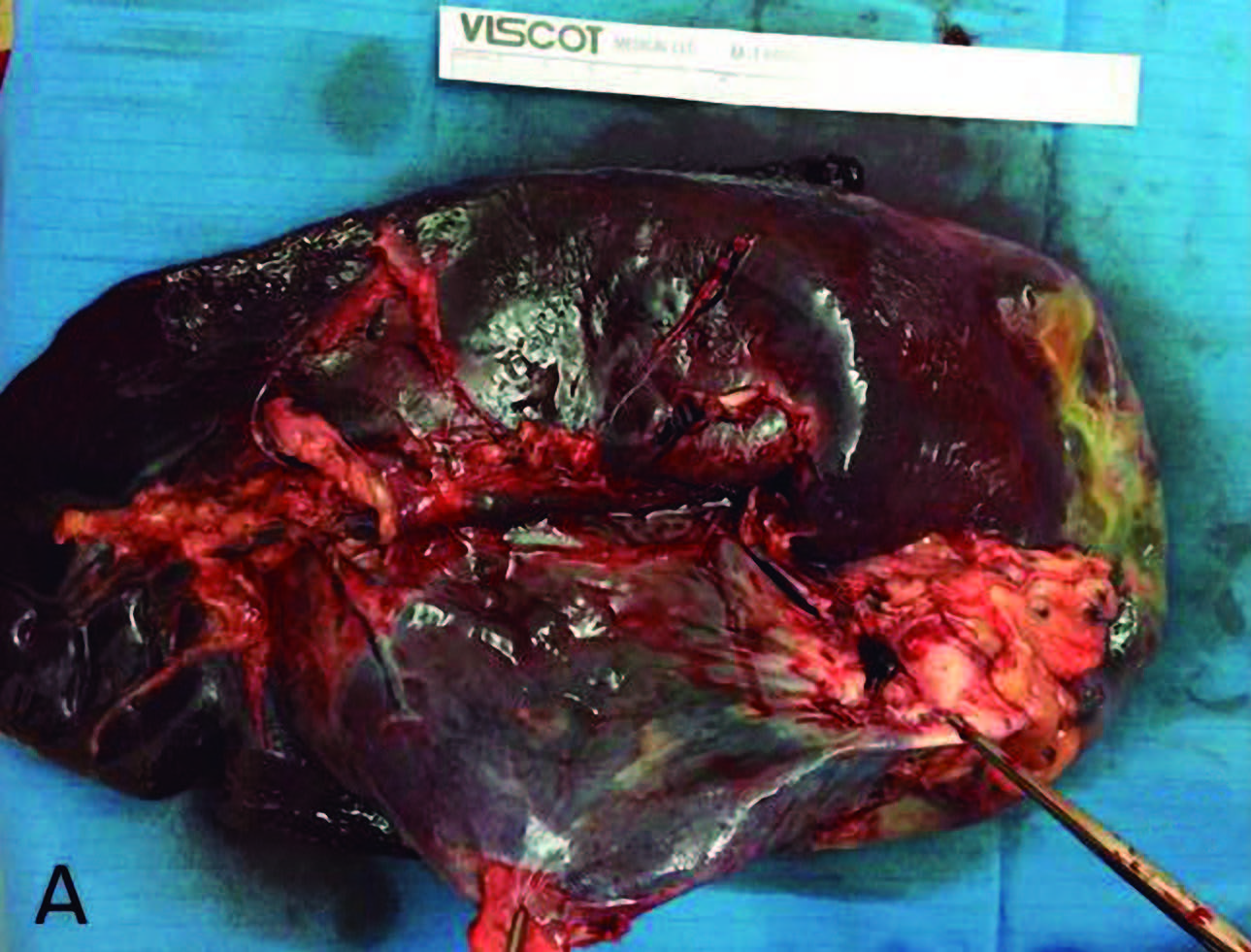
Figure 4. B. Microscopic vision with squamous epithelium of cystic wall lining.
Discussion
Cystic degeneration of the spleen is a rare entity and only 10% of these are true cysts. The definitive diagnosis is supported by histopathology findings of squamous cystic wall lining.
Ethology is unknown, however they are believed to be congenital metaplastic alterations that occur on early embryological age in the development of the splenic mesonephric tissue.8
Usually diagnosed in young women, these lesions can reach sizes up to 15 cm in diameter or more, but are mostly diagnosed as asymptomatic incidental imaging findings.4 In our first case, pain referred due to a car accident led to this finding, since there were no signs of acute complication such as bleeding, rupture or infection. In the second patient symptomatology was believed secondary to tumor mass effect.
Splenic cysts greater than 5 cm by imaging methods should be surgically resected, as they have an increased risk of complications such as spontaneous rupture, infection, or bleeding.9 Although nowadays the indication of total or partial splenectomy is controversial, tumors larger than 10 cm with elevated serum CA 19.9 antigen and/or hilum involvement should be resected by total splenectomy, to rule out malignant process and avoid recurrences.10,11
In both cases, the presence of a tumor on the upper pole and in intimate contact with the splenic hilum led the authors to consider total splenectomy as the choice of treatment.
Regarding the approach, laparoscopic surgery had shown better outcomes with improvements in morbidity rates, postoperative pain and early hospital discharge.12 In the presented cases, the patients were discharged on the second postoperative day and two years later they don’t show signs of recurrence.
There are several case reports that associate the presence of true splenic cyst with increase of serum tumor markers like CA 19.9. This oncologic marker is believed to be segregated by the cyst wall epithelium. The cystic fluid immunohistochemistry is usually positive for this antigen. In our cases only serological studies were performed with marker elevation (499 U/ml and 108 U/ml). There are no reports of elevation of this marker in other types of splenic cystic lesions, so these findings should increase suspicion of epidermoid cyst.
However, the possibility of an overgrowth malignant process should not be ruled out and other diagnosis test should be considered. Serological control at three months after surgery was found within normal values as expected.
In summary, benign epithelial splenic cyst is a rare congenital lesion, usually presented in young asymptomatic women with a serum Ca 19.9 elevation. Surgical resection continues to be the gold standard of treatment due to the risk of complications.
Laparoscopic approach for partial or total splenectomy is a good option in experienced surgeon hands, with good oncological outcomes, low complication rates and early hospital discharge.
Conflict of interest. No conflict to declare.
References
- Fowler RH. Nonparasitic benign cystic tumors of the spleen. Int Abstr Surg 1953; 96: 209-227.
- Martín JW. Congenital splenic cysts. Am J Surg 1958; 96: 302-308.
- Ingle SB, Hinge (Ingle) CR, Patrike S. Epithelial cysts of the spleen: a minireview. World J Gastroenterol 2014; 20: 13899-13903.
- Morgenstern L. Nonparasitic splenic cysts: pathogenesis, classification, and treatment. J Am Coll Surg 2002; 194: 306-314.
- Hoshino A, Nakamura Y, Suzuki H, Mizutani S, Chihara N, Matsunobu T, Maejima K, Miura K, Hanawa H, Nomura S, Toyoda T, Yamagishi S, Nakata R, Muraki A, Uchida E. Giant epidermoid cyst of the spleen with elevated CA 19-9 production managed laparoscopically: report of a case. J Nippon Med Sch 2013; 80: 470-474.
- Matsumoto S, Mori T, Miyoshi J, Imoto Y, Shinomiya H, Wada S, Nakao T, Shinohara H, Yoshida S, Izumi K, Okazaki J, Muguruma N, Takayama T. Huge splenic epidermoid cyst with elevation of serum CA19-9 level. J Med Invest 2015; 62: 89-92.
- Lobascio P, Carbotta G, Laforgia R, Fedele S, Sederino MG, Minafra M, Delvecchio A, Ferrarese F, Palasciano N. Total laparoscopic splenectomy for giant epidermoid cyst: a case report. G Chir 2017; 38: 202-204.
- Rana APS, Kaur M, Singh P, Malhotra S, Kuka AS. Splenic epidermoid cyst – a rare entity. J Clin Diagn Res 2014; 8: 175-176.
- Inokuma T, Minami S, Suga K, Kusano Y, Chiba K, Furukawa M. Spontaneously ruptured giant splenic cyst with elevated serum levels of CA 19-9, CA 125 and carcinoembryonic antigen. Case Rep Gastroenterol 2010; 4: 191-197.
- Tuqan NA, Saleeby GW. Primary reticulum-cell sarcoma of the spleen. Radiology 1959; 72: 868-871.
- Shuman RL, Bouterie RL. Cystadenocarcinoma of the pancreas presenting as a splenic cyst. Surgery 1976; 80: 652-654.
- Matsutani T, Uchida E, Yokoyama T, Matsushita A, Matsuda A, Sasajima K. Laparoscopic unroofing of a large pseudocyst of the spleen: report of a case. J Nippon Med Sch 2009; 76: 319-322.
Correspondencia: Santiago Reimondez
Naciones Unidas 346 (C.P.: 5000). Córdoba Capital, Argentina
Tel.: 54 – 0351 – 4688200 interno 865
Correo electrónico: santi_rei@hotmail.com
Acta Gastroenterol Latinoam 2019;49(1): 77-80
