
Franco José Signorini,1 Tomas Kruse,1 Verónica Gorodner,2 Pablo Sergio Maldonado,1 Lucio Ricardo Obeide,1 Federico Moser1
1 Departamento de Cirugía General, Hospital Privado Universitario de Córdoba. Córdoba.
2 Programa de Unidades Bariátricas. Ciudad Autónoma de Buenos Aires.
Argentina.
Acta Gastroenterol Latinoam 2019;49(1):81-86
Recibido: 24/11/2017 / Aprobado: 18/10/2018 / Publicado en www.actagastro.org el 18/03/2019

Summary
The splenic artery aneurysm is a rare entity, with a prevalence of less than 1%, but it is the most frequent among the visceral artery aneurysms. Nowadays the first treatment option is the endovascular when possible, although in some cases (large aneurysm, AV fistula, technical impossibility or complications of endovascular procedure) surgical approach indicated. In this study, we describe the laparoscopic approach for this pathology with and without splenectomy according to different scenarios. This procedure is feasible and safe in teams with vast laparoscopic experience.
Key words. Aneurysm, splenic artery, laparoscopic, spleen preserving, splenectomy.
Abordaje laparoscópico del aneurisma de la arteria esplénica
Reporte de tres casos y revisión de la literatura
Resumen
El aneurisma de la arteria esplénica es una entidad rara, con una prevalencia menor al 1%, pero es la más frecuente dentro de los aneurismas arteriales viscerales. En la actualidad la primera opción de tratamiento es la endovascular cuando sea posible, aunque en algunos casos (aneurismas de gran tamaño, fistulas arterio-venosas, imposibilidad técnica o complicaciones del procedimiento endovascular) el abordaje quirúrgico está indicado. En este estudio describimos el abordaje laparoscópico para esta patología con y sin esplenectomía de acuerdo con las diferentes situaciones. Este método es factible y seguro en equipos quirúrgicos con experiencia en laparoscopía.
Palabras claves. Aneurisma, arteria esplénica, laparoscópico, preservación esplénica, esplenectomía.
The splenic artery aneurysm defined as the presence of dilation greater than 1 cm in the diameter of the vessel, and the true aneurysm, which comprises the three layers of the wall (intima, media, adventitia), must be differentiated from the pseudo-aneurysm, consisting of only one or two layers.1
It is a rare entity, with a prevalence of less than 1%, but it is the most frequent (approximately 60% of the cases) among the visceral artery aneurysms.2 Its diagnosis is often difficult due to its nonspecific symptomatology. In some cases, its initial manifestation is rupture, causing haemorrhagic shock. It is more common in women with a ratio of 4:1, and related with multiparity.3 Although abdominal ultrasound has proved to be a useful diagnostic tool, the gold standard for diagnosis is a computed tomography (CT) of high resolution. Digital subtraction angiography reserved to the selected cases. Nowadays, the first treatment option is the endovascular treatment when possible, although in some cases (large aneurysm, AV fistula, technical impossibility or complications of endovascular procedure) surgical approach is indicated.4 We present three cases of splenic artery aneurysm demanding surgery that were approached laparoscopically.
Case serie and technique
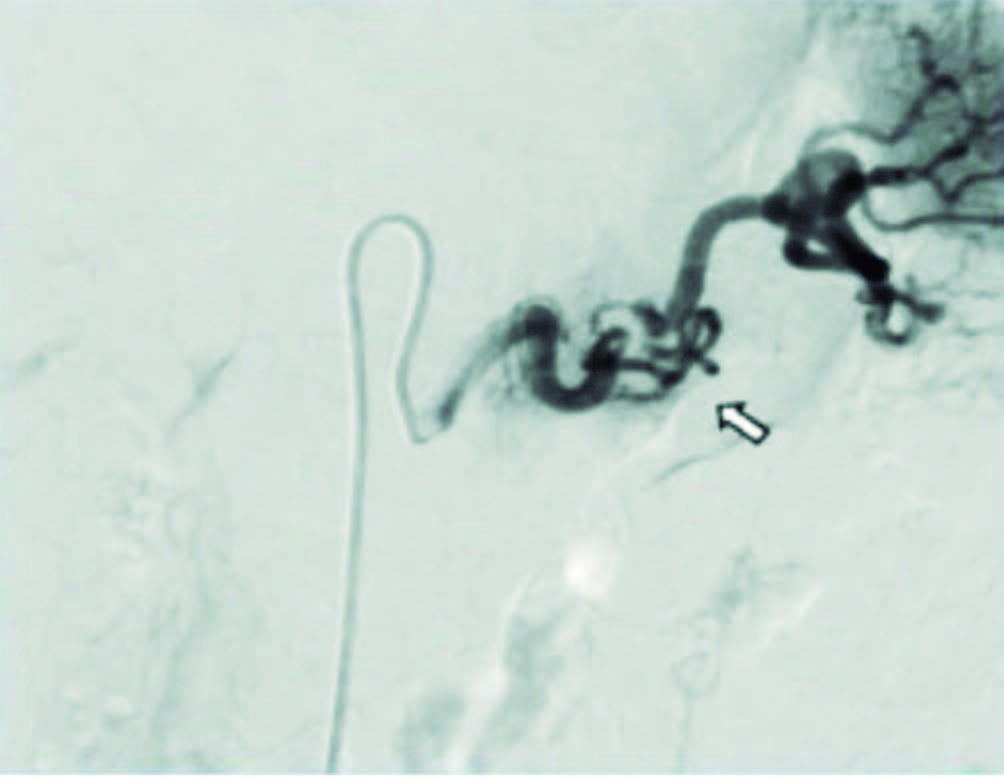
The first case was a 55-year-old female with no history of vascular disease, with 2 C-sections. In a context of suspected nephrolithiasis, the CT scan incidentally revealed a 28 mm splenic artery aneurysm in the middle third, with mural thrombosis. MR angiography (Figure 1) and selective arteriography (Figure 2) subsequently confirmed these findings. Due to the twisting path of the vessel accompanied by a moderate narrowing of the ostium of the celiac trunk and the presence of intra-arterial thrombosis, it was discarded the possibility of endovascular treatment and we opted for laparoscopic surgery. Position and preparation of the patient was identical in all cases: the patient placed in a 30° right lateral decubitus position. The surgeon positioned between the patient’s legs and the assistant towards the left side of the patient. The operation performed under general anaesthesia. The skin of the abdomen prepped and draped in the usual sterile fashion. Four trocars were used: a 12-mm trocar was placed in the midline supraumbilical position under direct vision using the Optiview® system, a 10-mm trocar was placed in the left flank (anterior axillary line), a 5-mm trocar in the right upper quadrant and another 5-mm in the left lower quadrant (mid axillary line). Entering the cavity, a tumour observed in the lesser sac nears the lesser curvature of the stomach. Splenic artery dissection was performed to the middle portion of the pancreas and it was possible to see the partially thrombosed aneurysm of 4 x 4 cm. By blunt maneuvers and harmonic scalpel dissection, the upper face of the pancreas dissected and a metallic vascular clamp placed immediately proximal to the aneurysm to observe the splenic vascularization. Dissection of the lesion with harmonic scalpel was completed (Figure 5) and the afferent and efferent artery of the aneurysm severed using vascular clips (Hemolog®). Good splenic perfusion confirmed by irrigation through collaterals previously studied by arteriography. The metal clamp removed and adhesions of the aneurysm to the splenic vein and small pancreatic vessels were resected using harmonic scalpel. Finally, the piece extracted through a 3 cm laparotomy in the subcostal trocar site. The postoperative period was uncomplicated and discharge was after 72 hours. At the annual clinical check-up, Doppler ultrasound showed no new vascular malformations and normal spleen vascularization. The progress was asymptomatic.
Figure 1. LMR angiography where the splenic artery aneurysm can be seen (case 1).
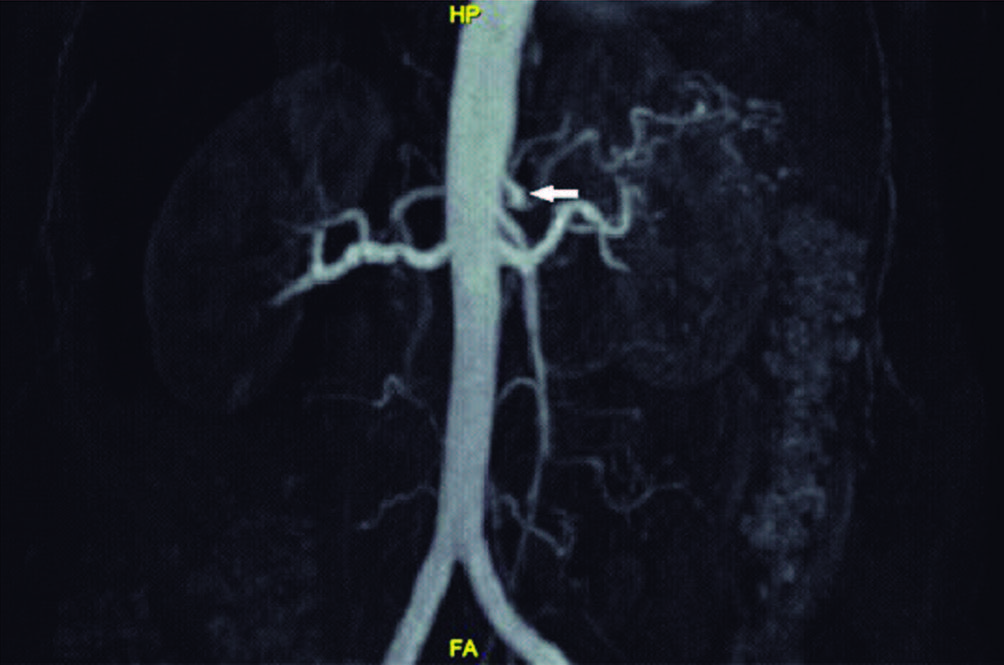
Figure 2. Selective angiography of the first case.
The second case was a female of 33 years, previously healthy. She consulted for nonspecific back pain and abdominal ultrasound performed finding dilation of the splenic artery. This finding confirmed with CT angiography (Figure 3) showing a dysplastic type abdominal aneurysm of 26 x 6 mm, with no evidence of complications. We initially opted for an endovascular treatment, which was complicated with the rupture of the aneurysm (CT scan showed retroperitoneal and intra-abdominal bleeding) and the need for hospitalization in intensive care unit. The complication was not associated with shock and intubation was not necessary. She responded well to a transfusion of one unit of red blood cells and fluid replacement with crystalloid. At the subsequent check-up, CT confirmed the persistence of the aneurysm. A new assessment performed and laparoscopic surgery was scheduled. Entering the cavity, we proceeded down the splenic flexure, separating the omental apron, followed by the opening of the lesser sac, sectioning the gastro colic ligament with harmonic scalpel. Splenic artery aneurysm observed in the rear part of the pancreas. We continued dislocating the spleen for better exposure, and then carefully dissected the splenic vein from splenic artery and from the aneurysm by ligation of efferent venous vessels from the arterial aneurysm. Dissection continued with the afferent and efferent branch of the splenic artery aneurysm and ultimate section of the aneurysm with 60 mm vascular stapling. The irrigation of the spleen was found unscathed. After careful haemostasis, the aneurysm removed from the abdominal cavity. The postoperative period passed favourably, with discharge 24 hours after the procedure. The clinical evolution was good, CT control at 6 months after surgery with no evidence of aneurysm.
Figure 3. CT angiography where dysplastic type abdominal aneurysm of 26×6 mm is depicted (case 2).

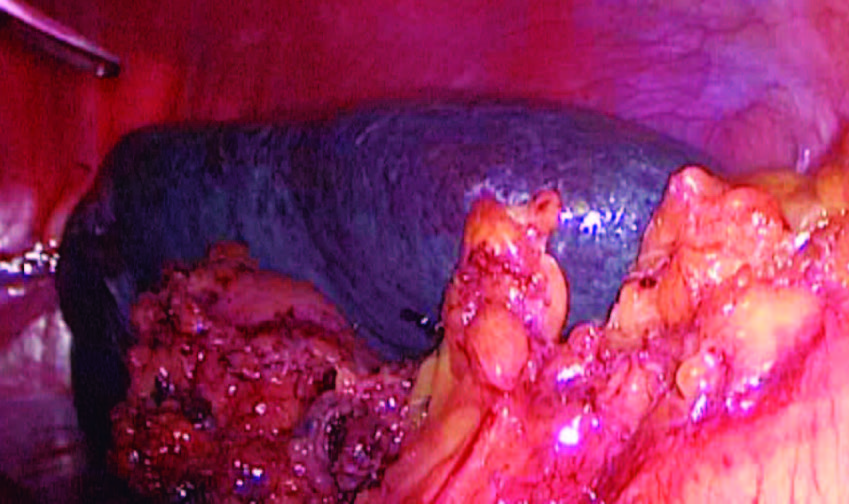
The third case was a 66-year-old male, type 2 diabetic with hypertension. In an annual clinical check-up, abdominal ultrasound (Figure 4) found a 30 mm saccular image in the lower polar branch of the splenic artery, corresponding to an aneurysm that, being partially thrombosed and very close to the splenic hilum, was excluded from endovascular treatment. Because it was also associated with central splenic infarction laparoscopic, approach decided. The mesocolon attached to the gastro-splenic omentum freed, using harmonic scalpel and then the gastrocolic omentum and lesser sac of the omentum opened, showing the tail of the pancreas. After careful dissection, we managed to find the splenic artery aneurysm of approximately 5 x 3 cm. Once the aneurysm released, clips placed on its afferent and efferent branches. Using a linear cutter stapler of 60 mm with white cartridge, it sectioned. After clipping, complete ischemia of the spleen observed (Figure 6) and therefore it decided to perform laparoscopic splenectomy. There was good post-operative evolution, with discharge at 72 hours. The subsequent clinical evolution was good.
Figure 4. 30 mm saccular image in the lower polar branch of the splenic artery is shown (case 3).
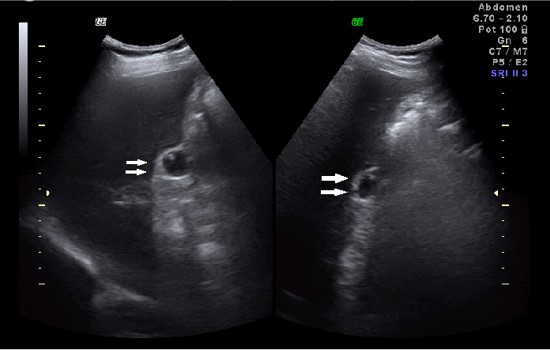
Figure 5. Splenic artery aneurysm dissected of the first case.

Figure 6. Spleen central and complete ischemia of the third case.

Discussion
Splenic artery aneurysm defined as the presence of expansion greater than 1 cm in the diameter of the vessel. The true aneurysm, comprising the three layers of the wall (intima, media, adventitia) must be differentiated from pseudo aneurysm, comprising only one or two of them (the latter is believed to be related to inflammatory processes like chronic pancreatitis).1
It presents rarely, with a prevalence between 0.1 and 0.2% (although in autopsies of individuals over 60 years, a prevalence of up to 10.4% has been recorded).2 Among intra-abdominal aneurysms, it is third in frequency behind those of the abdominal aorta and iliac arteries, and is the most frequent of the visceral aneurysms, covering 60% of these. It is more common in women, with a ratio of 4:1 compared to men, and is often associated with pregnancy (it is believed that this could be due to the hyperdynamic state and hormonal effects in the vessel wall) and with portal hypertension in cirrhosis patients.3
The diagnosis is often difficult due to nonspecific symptoms, and it may present with diffuse, dull abdominal pain, or pain located in the left upper quadrant. In some case, the initial manifestation could be rupture causing haemorrhagic shock. The diagnostic gold standard is CT, which enables arterial reconstruction and to appreciate its features, location, etc. Abdominal ultrasound is also very useful and is preferred in cases of patients admitted with ruptured aneurysm and hypovolemic shock for a rapid diagnosis of intraperitoneal bleeding located in the upper abdomen, ruling out other causes, particularly obstetric in pregnant patients where the differential diagnosis becomes even more difficult. Finally, Digital subtraction angiography reserved to the selected cases.5
Splenic artery aneurysms are indicated for treatment in the following situations: Symptomatic patients, asymptomatic with lesions > 2 cm, pregnant women or women of childbearing age with SAA > 1 cm. Lesions between 1 and 2 cm in asymptomatic patients should be monitored every 6 months to assess growth.6
Other authors consider that lesions in cirrhotic patients or candidates for liver transplantation must also be treated.2 The method of choice has traditionally been open surgery, although nowadays the use of endovascular techniques has begun to displace traditional surgery. Embolization can be performed by placing balls or «coils» within the aneurysmal sac, as well as placing endovascular stents; since the main complication is splenic infarction due to technical problems.7 Sticco et al. conducted a comparative study of cases of SAA, treated endovascular vs. conventional surgery. The results showed significant differences in the rates of cardiovascular and respiratory complications, which were higher in open surgical procedure, as well as a higher rate of surgical infections. The average hospitalization time was also higher for the open surgery group, but the in-hospital mortality rate was similar for both groups.8 Hogendoorn et al. performed a meta-analysis comparing the results found in endovascular methods, open surgery and conservative treatment. The result showed endovascular procedures with a lower rate of complications, including aneurysmal rupture, and lower rate of peri-operative mortality (follow-up at 30 days). However, this group presented a higher rate of long-term complications and need for reoperation.9
The laparoscopic approach in experienced surgeon hands is a simple, safe, minimally invasive technique with rapid recovery compared with open. Through this approach, the aneurysm could be ligated, resected, excluded or obliterated with or without splenectomy.10 Sometimes distal pancreatectomy is also required,11 the lateral approach may aid preservation of the short gastric collateral supply and to proceed to laparoscopic splenectomy if necessary. Most reports recommend this approach for distal aneurysm.12 On the other hand, if the aneurysm is located at the proximal third of the artery, splenic conservation should be attempted.13 The anterior approach can provide access to the proximal segment and the remainder of the intraabdominal cavity for concomitant procedures.10
In our experience, the first case approached laparoscopically as the artery was long and tortuous. In addition the presence of thrombosis promotes migration of the endovascular coil and recanalization of the pedicle aneurysm.14 Moreover, post-embolization syndrome reported in at least a third of cases and, although only a few patients require surgery for this reason because of splenic infarction it is, possible that many of them remain with a decreased splenic function. The ability of the laparoscopic approach to combine management of the splenic aneurysm with a possible concomitant splenectomy (as in the third case), prevents the development of this syndrome generated by splenic hypoperfusion.15
The use of the vascular clamp in this case had two aims: first, to ensure good splenic perfusion through the collaterals, and second, to enable good vascular control in case of a rupture of the aneurysm sac, because dissection is a delicate procedure and the sudden rupture of the thin wall of the aneurysm should always be feared.16
The only case, which addressed by endovascular route, suffered ruptured aneurysm as a complication intra procedure and required supportive measures and subsequent re-intervention with more expenses and hospital stay. In the third case, hemodynamic not indicated because the aneurysm was distal with a practically hilar location. In addition, the spleen already showed a central infarction and the embolization of the lesion without control of splenic perfusion was an unacceptable risk. The laparoscopic approach may thus be the choice in selected cases because of its good post-operative recovery and splenic control as well as the already mentioned contraindications for endovascular intervention.
Conclusions
To take into account, splenic artery aneurysm is a rare entity especially among high-risk groups (pregnant women and cirrhotic patients), because the complications of this disease carry a high rate of morbidity and mortality. An appropriate therapeutic method is essential. The endovascular approach considered the main choice but laparoscopic treatment should take place especially in cases where splenic perfusion is seriously threatened. Conventional surgery reserved only for hemodynamic emergency.
Conflicts of interest. None.
References
- Yagmur Y, Akbulut S, Gumus S, Demircan F. Giant splenic artery pseudoaneurysm: a case report and literature review. Int Surg 2015; 100: 1244-1248.
- Akbulut S, Otan E. Management of giant splenic artery aneurysm: comprehensive literature review. Medicine (Baltimore) 2015; 94: e1016.
- Davis T, Minardi J, Knight J, Larrabee H, Schaefer G. Ruptured splenic artery aneurysm: rare cause of shock diagnosed with bedside ultrasound. West J Emerg Med 2015; 16: 762-765.
- Wang CX, Guo SL, Han LN, Jie Y, Hu HD, Cheng JR, Yu M, Xiao YY, Yin T, Chu FT, Liang FQ. Computed tomography angiography in diagnosis and treatment of splenic artery aneurysm. Chin Med J 2016; 129: 367-369.
- Jackson HT, Diaconu SC, Maluso PJ, Abell B, Lee J. Ruptured splenic artery aneurysms and the use of an adapted fast protocol in reproductive age women with hemodynamic collapse: case series. Case Rep Emerg Med 2014; 2014: 454923.
- Pejkić _S, Tomić _I, Opačić _D, Pejinović _L, Grubor N, Činara I, Davidović Splenic artery aneurysms: two cases of varied etiology, clinical presentation and treatment outcome. Srp Arh Celok Lek 2015; 143: 326-331.
- Guang LJ, Wang JF, Wei BJ, Gao K, Huang Q, Zhai RY. Endovascular treatment of splenic artery aneurysm with a stent-graft: a case report. Medicine (Baltimore) 2015; 94: e2073.
- Sticco A, Aggarwal A, Shapiro M, Pratt A, Rissuci D, D’Ayala M. A comparison of open and endovascular treatment strategies for the management of splenic artery aneurysms. Vascular 2016; 24: 487-491.
- Hogendoorn W, Lavida A, Hunink MG, Moll FL, Geroulakos G, Muhs BE, Sumpio BE. Open repair, endovascular repair, and conservative management of true splenic artery aneurysms. J Vasc Surg 2014; 60: 1667-1676.
- Ha JF, Sieunarine K. Laparoscopic splenic artery aneurysm resection: review of current trends in management. Surg Laparosc Endosc Percutan Tech 2009; 19: e67-e70.
- Obuchi T, Sasaki A, Nakajima J, Nitta H, Otsuka K, Wakabayashi G. Laparoscopic surgery for splenic artery aneurysm. Surg Laparosc Endosc Percutan Tech 2009; 19: 338-340.
- Sandford RM, Lloyd DM, Ross Naylor A. Laparoscopic ligation of splenic artery aneurysm. Surg Laparosc Endosc Percutan Tech 2006; 16: 102-103.
- Barbaros U, Özemir IA, Aksakal N, Tükenmez M, Kiliç B, Ağcaoğlu O, Dinççağ _A, Seven R, Mercan S. Laparoscopic surgery of the splenic artery and vein aneurysm with spontaneous arteriovenous fistula. Surg Laparosc Endosc Percutan Tech 2013; 23: e127-e130.
- Gao BL, Li MH, Wang YL, Fang C. Delayed coil migration from a small wide-necked aneurysm after stent-assisted embolization: case report and literature review. Neuroradiology 2006; 48: 333- 337.
- Tsugawa K, Hashizume M, Tomikawa M, Tanoue K, Migou S, Sugimachi K. Laparoscopic splenectomy for splenic artery aneurysm. Hepatogastroenterology 1999; 46: 2631-2634.
- Pietrabissa A, Ferrari M, Berchiolli R, Morelli L, Pugliese L, Ferrari V, Mosca F. Laparoscopic treatment of splenic artery aneurysms. J Vasc Surg 2009; 50: 275-279.
Correspondencia: Tomás Kruse
Naciones Unidas 346 (C.P.: 5000). Departamento de cirugía general, Hospital Privado Universitario de Córdoba. Córdoba, Argentina
Tel: 00 54 351 6749838 – Tel/Fax: 00 54 351 4688200 (int. 865)
Correo electrónico: tomaskruse746@gmail.com
Acta Gastroenterol Latinoam 2019;49(1): 81-86
