Priscila R Armijo,1 Fernando PP Vicentine,1 Fernando AM Herbellar,1 Marco G Patti2
1 Department of Surgery, Escola Paulista de Medicina, Federal University of Sao Paulo. Sao Paulo, Brazil.
2 Department of Surgery, University of Chicago, Il. Chicago, EE.UU.
Acta Gastroenterol Latinoam 2016;46: 310-313
Recibido: 14/01/2016 / Aprobado: 12/10/2016 / Publicado en www.actagastro.org el 01/01/2017

Summary
Dysphagia after caustic ingestion may persist even after well-succeeded dilatation procedures and an open lumen suggesting other etiology for this symptom, such as dysmotility. Aims. This study aims to evaluate motility in a series of patients with previous esophageal stenosis after caustic ingestion at the light of high resolution manometry (HRM). Material and methods. Ten adult patients 5 women, mean age 54 (range: 28-83) years with previous esophageal caustic stenosis were recruited. The mean time from caustic ingestion to the esophageal test was 22 (range 6-45) months. All patients underwent successful endoscopic dilatation of the strictures and all of them were able to eat an unrestricted diet. Two (20%) patients complaint of mild dysphagia and 1 (10%) complaint of heartburn. All patients underwent a HRM. Results. Lower esophageal sphincter (LES) was defective in 8 (80%) patients with normal relaxation. Absence of peristalsis was present in 8 (80%) patients. Conclusion. Motility impairment was present in all patients with previous caustic ingestion that may explain dysphagia even when a mechanical obstruction is not detected by radiologic or endoscopic methods.
Key words. Caustic stenosis, motility, high resolution manometry, dysphagia, peristalsis, lower esophageal sphincter.
Evaluación con manometría de alta resolución de una cohorte de pacientes con antecedentes de estenosis esofágica por la ingesta de cáusticos
Resumen
La disfagia como consecuencia de la ingesta de cáusticos puede persistir incluso después de procedimientos exitosos de dilatación y con lumen abierto, lo que sugiere que otra etiología sea la responsable del síntoma como es la alteración de la motilidad del esófago. Objetivo. Evaluar la motilidad en una cohorte de pacientes con antecedentes de estenosis esofágica resultante de la ingesta de cáusticos mediante el uso de manometría de alta resolución (MAR). Material y métodos. Diez pacientes adultos, 5 mujeres, edad mediana: 54 años (rango: 28-83) con antecedentes de estenosis caústica esofágica fueron reclutados. El tiempo entre la ingesta de los cáusticos y la MAR fue de 22 meses (rango: 6-45). Todos los pacientes fueron sometidos a una dilatación endoscópica exitosa de las zonas con estenosis y eran capaces de comer una dieta sin restricciones. Dos pacientes (20%) presentaron disfagia leve y 1 de ellos (10%) presentó pirosis. Todos los pacientes fueron sometidos a MAR. Resultados. El esfínter esofágico inferior (EEI) fue defectuoso en 8 pacientes (80%) con relajación normal. El aperistaltismo estuvo presente en 8 pacientes (80%). Conclusión. Las alteraciones en la motilidad estuvieron presentes en todos los pacientes con antecedentes de ingesta de cáusticos, lo que podría explicar la disfagia, incluso cuando una obstrucción mecánica no es detectada por métodos radiológicos o endoscópicos.
Palabras claves. Estenosis cáustica, motilidad, manometría de alta resolución, disfagia, peristaltismo, esfínter esofágico inferior.
Caustic ingestion is a relevant public health problem in several countries. In the United States, from 5.000 to 15.000 caustic ingestions are estimated to occur per year.1 Esophageal stricture is a severe consequence of the corrosive ingestion leading frequently to repeated endoscopic dilations. However, dysphagia may persist even after well-succeeded dilatation procedures and an open lumen suggesting other etiology for this symptom.1, 2
Few previous studies focused on the esophageal motility by conventional manometry in patients after caustic ingestion.3, 4 High resolution manometry (HRM), however, seems to be a more adequate method for evaluation of these patients due to superior accuracy for the detection of incomplete lower esophageal sphincter (LES) relaxation and segmental peristalses defects.5, 6
This study aims to evaluate the motility in patients with esophageal stenosis after caustic ingestion at the light of HRM.
Material and methods
Population
Ten voluntary adult patients, median age: 54 years (range: 28-83), 50% females with esophageal caustic stenosis were recruited. Patients who refused to participate or with previous foregut operations were excluded from the study. The median time from caustic ingestion to the esophageal test was 22 months (range: 6-45).
All patients underwent successful endoscopic dilatation (no stenosis detected at the radiologic evaluation) of the strictures and all of them were able to eat an unrestricted diet. Two (20%) patients complaint of mild dysphagia and 1 (10%) complaint of heartburn.
Manometry
All patients underwent a HRM following previously described protocol.7 Medications that interferes with esophageal and gastric motility were discontinued 3 days before the study. HRM data of all volunteers were acquired using a solid-state HRM assembly with 36 sensors spaced at 1 cm intervals (Medtronics, Los Angeles, CA). All studies were performed with patients in sitting position, after a minimum fasting period of eight hours.
Position, pressure (defined as the mid-respiratory pressure), relaxation, and length of the lower esophageal sphincter (LES) were recorded. Esophageal body function was assessed by giving 10 wet swallows of 5 ml water boluses at 30-sec intervals when amplitude, duration and propagation of the peristaltic waves were assessed at 3 and 7 cm above the LES. Plots were manually reviewed for segmental defects of peristalsis. Upper esophageal sphincter (UES) pressure was also measured.
The normal values considered in this study were: LES length > 2.7cm, LES basal pressure 13-43 mmHg, LES residual pressure <15 mmHg, distal esophageal amplitude (DEA) (sensor located 3 cm above the upper border of the LES) 41-168 mmHg and proximal esophageal amplitude (PEA) (sensor located 7cm above the upper border of the LES) 37-166 mmHg, UES basal pressure 34-104 mmHg, and UES residual pressure <12 mmHg. Distal contractile integral (DCI) defined esophageal contractions as ineffective (failed + weak) if < 800 mmHg.s.cm or hypercontractile if > 8.000 mmHg.s.cm and distal latency (DL) < 4.5s defined a premature contraction.8
Analysis statistics
Variables are expressed as mean ± standard deviation. Shapiro-Wilk test was used to assess normal distribution of variables. Only DCI had a non-normal distribution (w = 0.76, p < 0.01), thus parametric tests were used. Fisher exact test was used for analysis of contingency of categorical variables (frequency of hypotonic LES, absence of peristalsis and ineffective contractions) and Student T tests was used for comparison of means (LES length and pressure, DCI, DL) p < 0.05 was considered significant.
Ethics
This study was approved by the Research Ethics Committee of the Sao Paulo Federal University. All patients signed an informed consent. There were no conflicts of interest. The authors are responsible for the manuscript; no ghost or professional writer was hired.
Results
Lower Esophageal Sphincter
Manometric LES parameters are depicted in Table 1. LES was short in 7 (70%) patients and hypotonic in 5 (50%). LES was defective (short or hypotonic) in 8 (80%). LES relaxation was normal in all patients.
Esophageal body
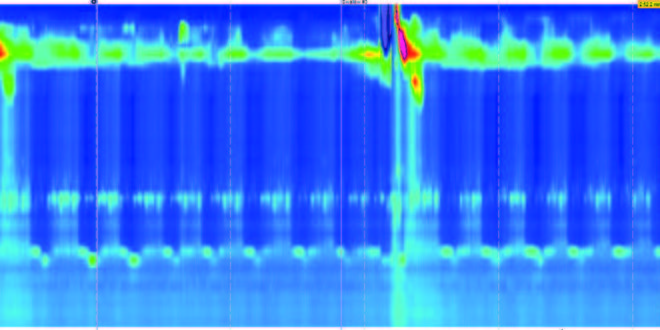
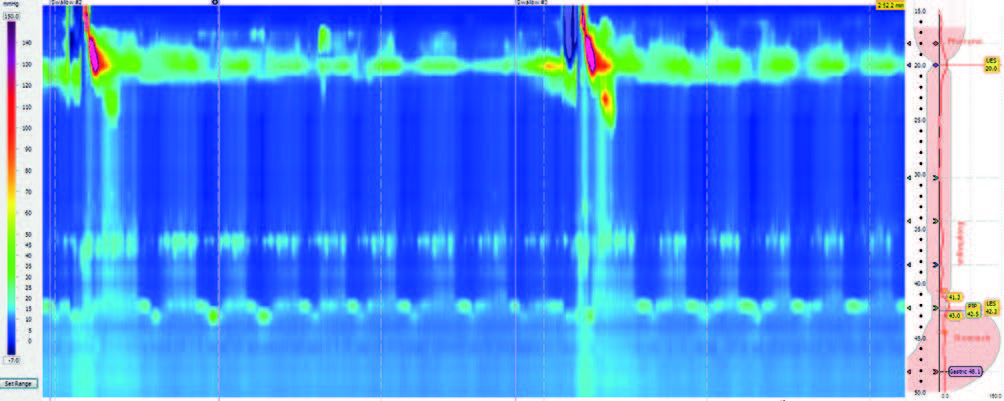
Manometric parameters for the esophageal body are described in Table 1. Absence of peristalsis was present in 8 (80%) patients (Figure 1). DCI was abnormal (ineffective) in 70% of the patients. Seven (70%) patients had premature contractions, measured by the DL.
According to the Chicago Classification 3.0,8 8 (80%) were classified as “absent contractility”, 1 (10%) as ineffective motility and 1 (10%) not classified in any named motility disorder.
Table 1. Manometric parameters in patients after caustic ingestion (n = 10).
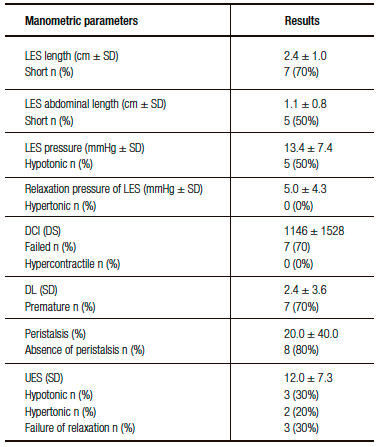
Figure 1. High-resolution manometry in a patient after caustic ingestion depicting absence of peristalsis.
Upper Esophageal Sphincter
Manometric UES parameters are depicted in Table 1. UES was hypotonic in 3 (30%) patients and hypertonic in 2 (20%).
Symptoms
LES length was normal in all patients with dysphagia that present a longer LES length compared to patients without dysphagia (p = 0.03). LES basal pressure was normal in all patients with dysphagia with pressure (p = 0.3) and the % of hypotonic LES (p = 0.5) similar between patients with dysphagia or not. LES residual pressure was similar between groups (p = 0.4).
A higher frequency of absence of peristalsis was noticed in patients with dysphagia (p = 0.0001). Patients with dysphagia had higher DCI (p = 0.001) but with a similar distribution of ineffective contractions (p = 0.07) and DL (p = 0.5) in comparison with patients without dysphagia. UES pressure (p = 0.2) was similar in both groups.
Discussion
Our results show that esophageal motility after caustic ingestions is characterized by a significant percentage of defective LES and absence of peristalsis. Dysphagia is more prevalent in patients with absence of peristalsis.
Lower Esophageal Sphincter
Caustic ingestion may affect not only the mucosa but lead to necrosis and subsequent fibrosis of the muscular layer as well.9 Thus, we hypothesized that the LES could also be affected causing a loss of distensibility and failure of relaxation. Our results do not support this theory since LES relaxation was normal. Dysphagia was not correlated to any LES manometric parameter.
On the other hand, our data showed a significant number of patients with a defective LES, either due to hypotonicity or inadequate length. Previous studies with conventional manometry also showed low LES resting pressure.3, 4 Although patients were not tested for gastroesophageal reflux disease (GERD) in our studies and in previous series, the presence of a defective LES may lead to GERD resulting in re-stenosis after successful endoscopic dilatation.10 Heartburn was present in only 10% of our patients precluding statistical analysis with manometric parameters.
Esophageal body
Previous studies with conventional manometry showed a high prevalence of aperistaltic contractions after caustic ingestion even in asymptomatic patients.3, 4 HRM analysis of these patients also showed a significant number of absence of peristalsis.8 More sophisticated HRM parameters, including the DCI and DL,8 were used in our analysis. Distal esophageal contractile vigor is summarized using the DCI. This parameter applies an algorithm to quantify the contractile pressure exceeding 20 mmHg for the region spanning from the transition zone to the proximal aspect of the LES.8 It was initially devised to differentiate hypercontractility from normal contractions, but has subsequently been adapted to identify hypocontractile conditions as well.8 DL is a more objective parameter to define wave velocity and its correlation to swallowing in order to define premature (previously simultaneous) contractions. In our series, DCI was normal in only 30% of the cases but in these cases peristalsis was absent and DL abnormal. This finding shows that abnormal motility, either based on amplitude or coordination, is defective in all patients after caustic ingestion.
Dysphagia correlated with absence of peristalsis and a higher DCI. This finding implies that motility impairment can be a putative factor in the cause and maintenance of this symptom even in patients with treated stenosis.
Upper Esophageal Sphincter
Caustic ingestion may damage upper airways and the proximal esophagus.11-13 Our data showed an erratic distribution of UES pressure and relaxation that do not correlate with dysphagia.
Conclusion
Our series comprises a small number of patients; however, it is the first time that HRM was used to evaluate motility after caustic ingestion in patients after treated esophageal stenosis. Our results showed that LES becomes defective in most patients. Motility impairment is present in all patients that may explain dysphagia even when a mechanical obstruction is not detected by radiologic or endoscopic methods.
Acknowledgements. We are indebted to Ms. Vanessa Horich Tuxen for her invaluable assistance with the esophageal tests.
Author’s contribution.
PRA: acquisition of data, analysis and interpretation of data, drafting the article, final approval of the version to be published.
FPPV: acquisition of data, analysis and interpretation of data, drafting the article, final approval of the version to be published.
FAMH: conception and design, acquisition of data, analysis and interpretation of data, drafting the article, review for intellectual content, final approval of the version to be published.
MGP: review for intellectual content, final approval of the version to be published.
Supportive foundations. none.
Data sharing statement. Technical appendix, statistical code, and dataset available from the corresponding author at herbella.dcir@epm.br
Referencias
- Lupa M, Magne J, Guarisco JL, Amedee R. Update on the diagnosis and treatment of caustic ingestion. Ochsner J 2009; 9: 54-59.
- Harlak A, Yigit T, Coskun K, Ozer T, Mentes O, Gülec B, Kozak O. Surgical treatment of caustic esophageal strictures in adults. Int J Surg 2013; 11: 164-168.
- Dantas RO, Mamede RC. Esophageal motility in patients with esophageal caustic injury. Am J Gastroenterol 1996; 91: 1157- 1161.
- Moody FG, Garrte JM. Esophageal achalasia following lye ingestion. Ann Surg 1969; 170: 775-784.
- Kahrilas PJ, Peters JH. Evaluation of the esophagogastric junction using high resolution manometry and esophageal pressure topography. Neurogastroenterol Motil 2012; 24: 11-19.
- Vicentine FP, Herbella FA, Silva LC, Patti MG. High resolution manometry findings in patients with esophageal epiphrenic diverticula. Am Surg 2011; 77: 1661-1664.
- Vicentine FP, Herbella FA, Allaix ME, Silva LC, Patti MG. High resolution manometry classifications for idiopathic achalasia in patients with chagas’ disease esophagopathy. J Gastrointest Surg 2014; 18: 221-224.
- Kahrilas PJ, Bredenoord AJ, Fox M, Gyawali CP, Roman S, Smout AJ, Pandolfino JE. International high resolution manometry working group. The Chicago classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil 2015; 27: 160-174.
- Butler C, Madden JW, Davis WM, Peacock EE Jr. Morphologic aspects of experimental esophageal lye strictures. II. Effect of steroid hormones, bougienage, and induced lathyrism on acute lye burns. Surgery 1977; 81: 431-435.
- Cakal B, Akbal E, Köklü S, Babalı A, Koçak E, Taş A. Acute therapy with intravenous omeprazole on caustic esophageal injury: a prospective case series dis esophagus 2013; 26: 22-26.
- Benjamin B, Agueb R, Vuarnesson H, Tranchart H, Bongrand NM, Sarfati E, Cattan P, Chirica M. Tracheobronchial necrosis after caustic ingestion. Ann Surg 2016; 263: 808-813.
- Chiba S, Brichkov I. Pulmonary patch repair of tracheobronchial necrosis with perforation secondary to caustic ingestion. Ann Thorac Surg 2014; 97: 2205-2207.
- Jaillard S, Nseir S, Métois D, Marquette CH, Darras J, Porte H, Wurtz A.extensive corrosive injuries of the upper airways and gastrointestinal tract. J Thorac Cardiovasc Surg 2002; 123: 186-188.
Correspondencia: Fernando AM Herbella
Department of Surgery, Escola Paulista de Medicina
Rua Diogo de Faria 1087 cj 301, 04037-003. Sao Paulo, SP, Brazil
Tel.: +55-11-99922824
Correo electrónico: herbella.dcir@epm.br
Acta Gastroenterol Latinoam 2016;46(4): 310-313
