Fernanda Kara Carmo1 ID· Francisca Santorcuato Cubillos2 ID· Ignacio Maldonado Schoijet3 ID
1 Radiology resident, Facultad de Medicina Universidad de los Andes, Clínica Dávila, Santiago, Chile.
2 Medical Student, Facultad de Medicina Universidad de los Andes, Clínica Dávila, Santiago, Chile.
3 Body Imaging Radiologist, Associate Professor of Radiology, Facultad de Medicina Universidad de Los Andes, Clínica Dávila, Santiago, Chile.
Acta Gastroenterol Latinoam 2023;53(2):188-192
Received: 30/03/2023 / Accepted: 12/06/2023 / Published online: 30/06/2023 / https://doi.org/10.52787/agl.v53i2.313

Summary
In the emergency setting, right lower quadrant pain is a common clinical scenario. While acute appendicitis is the most relevant cause, there is a wide differential diagnosis. Valentino syndrome is a rare entity in which gastric or duodenal perforation, usually secondary to peptic ulcer disease, presents clinically with right lower quadrant pain mimicking acute appendicitis. It has its origins in Rudolph Valentino, a famous American actor who died of sepsis following an undiagnosed perforated ulcer after an appendectomy. Nowadays, radiological images play a crucial role in this pathology, historically diagnosed using exploratory laparotomy. Through a clinical case and a review of the literature, we aim to describe the historical evolution of Valentino’s syndrome, illustrate its clinical and radiological characteristics and highlight the increasing role of imaging, particularly computed tomography, in its early prospective diagnosis and in guiding targeted treatment. Finally, it is important to consider this pathology when assessing acute abdominal patients with coexisting pneumoperitoneum and appendicitis.
Keywords. Computed tomography, appendicitis, acute abdomen, peptic ulcer perforation, peritonitis, right lower quadrant pain, Valentino’s syndrome.
Síndrome de Valentino: de la historia a las imágenes. Revisión de la literatura basada en un caso clínico
Resumen
En el ámbito de urgencias el dolor en fosa ilíaca derecha es un cuadro clínico frecuente. Aunque la apendicitis aguda es la causa más relevante, existen otros diagnósticos diferenciales. El síndrome de Valentino es una patología infrecuente en la que una perforación gástrica o duodenal, generalmente secundaria a enfermedad ulcerosa péptica, se presenta clínicamente con dolor en el cuadrante inferior derecho, simulando una apendicitis aguda. Tiene su origen en Rudolph Valentino, un famoso actor estadounidense que murió de sepsis secundaria a una úlcera perforada no diagnosticada luego de una apendicectomía. Actualmente, las imágenes radiológicas tienen un papel fundamental en esta patología, históricamente diagnosticada mediante laparotomía exploradora. A través de un caso clínico y la revisión bibliográfica, nuestro objetivo es describir la evolución del síndrome de Valentino, ilustrar sus características clínico-radiológicas y destacar el papel cada vez más importante de las imágenes, especialmente la tomografía computada, para su diagnóstico prospectivo temprano y para orientar el tratamiento dirigido. Finalmente, es importante considerar esta patología en la evaluación de pacientes con abdomen agudo en los que coexisten neumoperitoneo y apendicitis.
Palabras claves. Tomografía computada, apendicitis, abdomen agudo, perforación úlcera péptica, peritonitis, dolor fosa ilíaca derecha, síndrome de Valentino.
Abbreviations
CT: computed tomography.
NSAIDs: non-steroidal anti-inflammatory drugs.
Introduction
Valentino´s syndrome is a rare pathology caused by irritation of the peritoneum due to fluid from a perforated ulcer migrating into the paracolic sulcus.1 This condition may mimic acute appendicitis or other differential diagnoses of right lower quadrant pain such as ureteral colic, diverticulitis, diverticulum rupture, ovarian torsion, ruptured ectopic pregnancy, perforated cholecystitis, pancreatitis, and pelvic inflammatory disease.2- 4
This entity requires surgical resolution.5 Correct and timely diagnosis is important because delay in treatment can increase morbidity and mortality.1 However, prospective diagnosis based on imaging can be challenging. The main risk factors for peptic ulcers, such as overuse of NSAIDs, Helicobacter pylori infection, tobacco, stress, and irregular or unhealthy eating habits, among others, should be taken into account.3 In this context, we aim to make a historical review of Valentino´s syndrome, highlight the role of computed tomography (CT), and provide key points for the early diagnosis of this entity.
Case Report
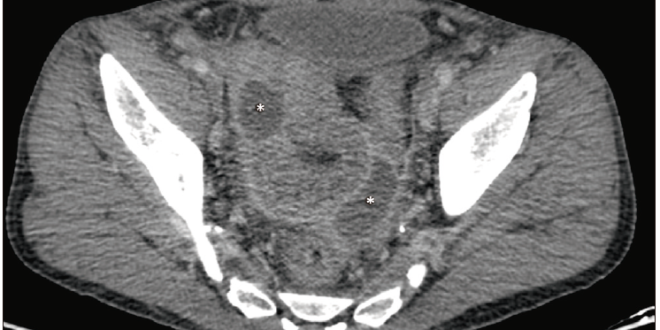
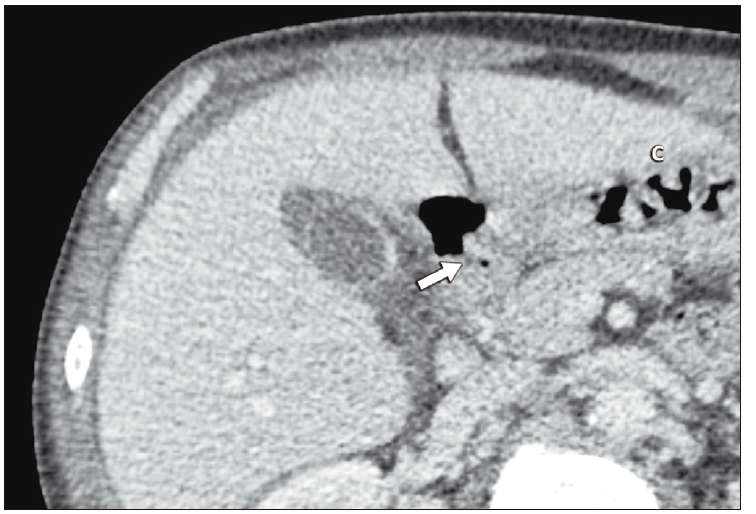
We present the case of a 52-year-old man with no known medical history who presented with a one-week history of right lower quadrant abdominal pain, a positive Blumberg sign on physical examination and elevated inflammatory parameters on laboratory tests. CT showed extensive diffuse intra-abdominal inflammatory changes with collections in the right iliac fossa (Figure 1) adjacent to the cecal appendix and distal ileum (Figure 2). There was also supramesocolic pneumoperitoneum (Figure 2 and 3), a subhepatic collection adjacent to the antral region containing fluid and gas, and an apparent focal discontinuity in the anterior wall of the pylorus (Figure 3).
Figure 1. Axial CT, portal phase. Extensive peritoneal inflammatory changes in the pelvic cavity with two abscesses (*)
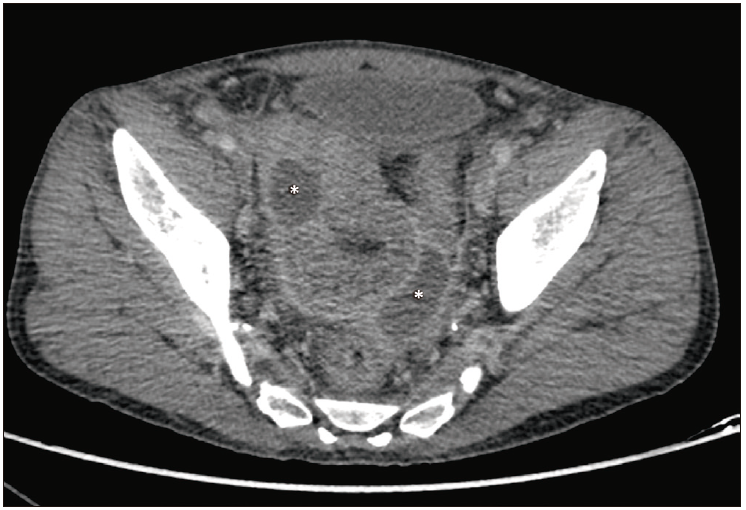
Figure 2. Coronal CT, portal phase. Inflammatory changes in the right iliac fossa (arrow) with collections (*), and pneumoperitoneum adjacent to the pylorus (arrowhead)

Figure 3. Axial CT, portal phase. Focal parietal discontinuity in the pyloric region (arrow), with adjacent pneumoperitoneum
The subsequent laparotomy confirmed a pyloric gastric perforation with secondary ileal and appendicular inflammatory changes, and included perforation of the appendix and distal ileum, all of which were surgically treated with ileal resection and gastric repair (Figure 4).
Figure 4. Surgical specimen of right hemicolectomy and ileum. Note the dark wall of the cecum representing transmural wall necrosis

The patient had a favourable clinical course with postoperative antibiotic treatment, without further complications and was discharged after two weeks.
Discussion
Acute abdominal pain is one of the most common presenting symptoms in the emergency department, with a broad differential diagnosis ranging from benign and self-limited entities to pathologies with high mortality that more often requires surgery. The initial clinical approach attempts to narrow the differential diagnosis by anatomical regions, dividing the abdomen into quadrants. The main objective is to identify pathologies that require surgical intervention, such as acute appendicitis, and to differentiate them from non-surgical entities that can be managed conservatively. Clinical characteristics, laboratory parameters, and imaging are often used in this approach.
Although acute appendicitis is one of the most relevant and common pathologies to consider in the setting of right lower quadrant pain, there is a wide range of clinical mimics, including acute right colonic diverticulitis, Meckel´s diverticulitis, ileitis, colitis and even renal colic.
In women, gynecological causes such as ovarian torsion, ruptured ectopic pregnancy, pelvic inflammatory disease, or endometriosis should be considered.4
Valentino´s syndrome is a rare condition in which a gastric or duodenal ulcer mimics acute appendicitis, usually secondary to complicated peptic ulcer disease.1
This entity originates from Rudolph Valentino (Rodolfo Pietro Filiberto Raffaello Gugliemi di Valentina d`Antonguolla), an Italian actor based in the United States who starred in several well-known silent films of the 1920s. Known in Hollywood as the “Latin Lover”, he died in 1926 at the age of 31 from septic complications (peritonitis and pleuritis) of an undiagnosed perforated peptic gastroduodenal ulcer. This ulcer simulated appendicular abdominal pain and was treated surgically with an appendectomy, the final diagnosis being made at autopsy.2
Few cases are reported in the literature, with the most comprehensive review published in 2022, consisting of 31 patients.3 Its exact incidence and prevalence are unknown. Although this is an extremely rare presentation of peptic ulcer disease, it is highly relevant because it can be life-threatening if not treated correctly and promptly. Therefore, high suspicion and accurate diagnosis are required.
The peptic ulcer disease has a complex and multifactorial pathophysiology, including alteration of protective factors (prostaglandins) and aggravating factors (hydrochloric acid), resulting in gastric or duodenal mucosal necrosis. Known etiological factors include the presence of Helicobacter pylori , the use of non-steroidal anti-inflammatory drugs (NSAIDs), smoking, and less common conditiones such as Zollinger-Ellison disease, Crohn´s disease, and Behcet´s disease, among others.4 Peptic ulcer disease typically presents with upper abdominal pain that may improve with food and, in more severe cases, may be complicated by bleeding or obstruction of gastric emptying. In cases of a transmural perforation, it may present as an acute abdomen with signs of peritonitis. When gastric or duodenal intraluminal fluid, leaks into the right iliac fossa in the setting of a perforation, it can cause focal peritonitis simulating acute appendicitis, including secondary appendicitis, explaining the clinical features of Valentino´s syndrome. It may be associated with pneumoperitoneum or pneumoretroperitoneum, depending on the location of the perforation.6
Previously, this diagnosis was made during surgery in a patient with a suspected case of appendicitis in whom a normal appendix was found. After an intraperitoneal search, a gastroduodenal ulcer was detected.
Currently, contrast-enhanced CT of the abdomen and pelvis is considered the study of choice for the prospective diagnosis of Valentino´s syndrome and, according to the literature, is the most commonly used method, to make the diagnosis in more than 70% of cases. CT is particularly useful in detecting pneumoretroperitoneum in the setting of duodenal perforation. It is more sensitive in detecting pneumoperitoneum than other techniques such as abdominal radiography.
CT findings in Valentino´s syndrome are gastric or duodenal wall thickening, fat stranding or inflammatory changes in the adjacent regions, and occasionally the perforation site may be seen. Frequently, collections can be seen either perigastric, periduodenal, retroperitoneal, or in the right iliac fossa, often associated with moderate pneumoperitoneum or pneumoretroperitoneum.
After detection and characterisation by CT, this entity can be confirmed and treated surgically by open or laparoscopic techniques, sealing the defect.
In this clinical case, a striking fact on the CT, otherwise rare, is the coexistence of an extensive peritoneal inflammatory process centred on the right iliac fossa with involvement of the appendix and distal ileum, added to a moderate supramesocolic pneumoperitoneum in the context of gastric perforation, suggesting two independent events. The lesson of this case is that there may be a pelvic peritoneal inflammatory process with secondary appendiceal involvement due to perforation of the upper hollow viscus (stomach and duodenum), and this syndrome should be suspected in the face of apparent primary appendicitis complicated by a significant supramesocolic predominance of the pneumoperitoneum, particularly in cases where the solution of continuity of the gastric or duodenal wall is not so evident.
In the case of a gastric ulcer, biopsies are recommended to rule out malignancy. Eradication therapy for Helicobacter pylori is also recommended.
Appropriate and prompt surgical treatment reduces the morbidity and mortality of this condition, whereas delayed treatment increases the risk of infectious complications and treatment failure.1 This highlights the importance of knowing this rare entity in order to make a prospective and prompt diagnosis when necessary.2
Conclusion
Valentino’s syndrome is a rare but important entity in which radiologists play a critical role in its early and accurate prospective diagnosis. Contrast-enhanced CT is considered the modality of choice in the detection and characterisation of this entity, and radiologists should have a high index of suspicion for signs of gastroduodenal inflammation in the setting of right lower quadrant pain.
Consent for publication. Anonymized data were used for the elaboration of this article, which did not distort its scientific value.
Intellectual Property. The authors declare that the data and figures presented in the manuscript are original and were carried out at their belonging institution.
Funding. The authors declare that there were no external sources of funding.
Conflict of interest. The authors declare that they have no conflicts of interest in relation to this article.
Copyright

© 2023 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Kara Carmo F, Santorcuato Cubillos F, Maldonado Schoijet I. Valentino’s Syndrome: from History to Images. A Case-based Literature Review. Acta Gastroenterol Latinoam. 2023;53(2):188-192. https://doi.org/10.52787/agl.v53i2.313
References
- Noussios G, Galanis N, Konstantinidis S, Mirelis C, Chatzis I, Katsourakis A. Valentino’s syndrome (with retroperitoneal ulcer perforation): A rare clinical-anatomical entity. Am J Case Rep [Internet]. 2020;21:e922647. http://dx.doi.org/10.12659/AJCR.922647
- Wijegoonewardene SI, Stein J, Cooke D, Tien A. Valentino’s syndrome a perforated peptic ulcer mimicking acute appendicitis. BMJ Case Rep [Internet]. 2012;2012(jun28 1):bcr0320126015-bcr0320126015. http://dx.doi.org/10.1136/bcr.03.2012.6015
- Mahajan PS, Abdulmajeed H, Aljafari A, Kolleri JJ, Dawdi SA, Mohammed H. A cautionary tale: Unveiling Valentino’s syndrome. Cureus [Internet]. 2022;14(2):e22667. http://dx.doi.org/10.7759/cureus.22667
- Toprak H, Yilmaz TF, Yildiz S, Turkmen I, Kurtcan S. Mimics of acute appendicitis-alternative diagnoses at sonography, CT, and MRI; specific imaging findings that can help in the differential diagnosis. Clinical Imaging. 2018;48:90-105. DOI:10.1016/j.clinimag.2017.10.001
- Amann C, Austin A, Rudinsky S. Valentino’s syndrome: A life-threatening mimic of acute appendicitis. Clin Pract Cases Emerg Med [Internet]. 2017;1(1):44-6. http://dx.doi.org/
10.5811/cpcem.2016.11.32571 - Mahajan PS, Abdalla MF, Purayil NK. First report of preoperative imaging diagnosis of a surgically confirmed case of Valentino’s syndrome. Journal of Clinical Imaging Science. 2014;4:28. DOI:10.4103/2156-7514.133263
Correspondence: Ignacio Maldonado Schoijet.
Email: Imschoijet@gmail.com
Acta Gastroenterol Latinoam 2023;53(2):188-192
