Julia R Kalluf,1 Fernando A M Herbella,1 Fernanda M Lafraia,1 Francisco Schlottmann,2 Marco G Patti2
1 Department of Surgery, Federal University of São Paulo, São Paulo, Brazil.
2 Department of Surgery, University of North Carolina, Chapel Hill, United States.
Acta Gastroenterol Latinoam 2019;49(4):331-335
Recibido: 21/06/2018 / Aprobado: 15/05/2019 / Publicado en www.actagastro.org el 17/12/2019

Summary
Symptoms have a low accuracy for the diagnosis of gastroesophageal reflux disease (GERD) compared to pH monitoring. The absence of GERD in patients with reflux symptoms can be explained by esophageal dysmotility, visceral hypersensitivity, hypervigilance and psychosocial characteristics. The number of symptoms experienced in 24 hours may represent some of these functional, sensorial and psychosocial characteristics. Aims. This study aims is to correlate the number of symptoms reported during 24-hour pH monitoring with the diagnosis of GERD. Methods. We studied 424 non-selected patients (58% females, median age 41 years, range 18-77) that underwent a pH monitoring for suspected GERD. Esophageal symptoms, extraesophageal symptoms, and no symptoms were reported in 199 (47%), 129 (30%), and 150 (35%) of the tests, respectively. Patients were grouped in GERD + and GERD – according to the DeMeester score. Symptom association was defined by the Symptom Index. Results. GERD + comprised 180 (44%) patients. Total number of symptoms, number of esophageal and extraesophageal symptoms, and symptom index were higher in patients GERD +. Symptoms and DeMeester score did not correlate for the total number of symptoms, esophageal symptoms, extraesophageal symptoms and symptom index. Conclusion. In conclusion, GERD + patients reported higher number of symptoms during pHmonitoring but the number of symptoms is not a good predictor for GERD presence or severity.
Key words. Gastroesophageal reflux disease, Esophageal pH monitoring, Symptoms, DeMeester Score, Hypervigilance.
Pronóstico del número de síntomas durante la pHmetría para el diagnóstico de la enfermedad por reflujo gastroesofágico
Resumen
Los síntomas poseen baja precisión para el diagnóstico de la enfermedad por reflujo gastroesofágico (ERGE) en comparación con la pHmetría esofágica. La ausencia de ERGE en pacientes con síntomas de reflujo puede ser explicada por las alteraciones en la motilidad esofágica, hipersensibilidad visceral, hipervigilancia o características psicosociales. El número de síntomas dentro de las 24 horas puede representar algunas de estas características funcionales, sensoriales y psicológicas. Objetivos. Correlacionar el número de síntomas reportados durante la pHmetría con el diagnóstico de ERGE. Métodos. Realizamos una pHmetría en 424 pacientes aleatorios (58% mujeres, edad mediana: 41 años; rango: 18-77) con sospecha de ERGE. Síntomas esofágicos, extraesofágicos y ausencia de síntomas estuvieron presentes en 199 (47%), 129 (30%), y 150 (35%), respectivamente. Los pacientes fueran agrupados en ERGE + y ERGE – de acuerdo con el índice de DeMeester. La asociación entre los síntomas y los episodios de reflujo fue definida por el “Índice Sintomático”. Resultados. 180 (44%) pacientes fueron diagnosticados con ERGE +. El número total de síntomas, número de síntomas esofágicos y extraesofágicos y el índice de síntomas fueran mayores en los pacientes con ERGE +. Síntomas y el Índice de DeMeester no se correlacionaron con el número de síntomas total, esofágicos o extraesofágicos y el “Índice Sintomático”. Conclusiones. Los pacientes con ERGE + reportaron un número mayor de síntomas durante la pHmetría, pero el número de síntomas no es un buen predictor de la presencia o severidad de la ERGE.
Palabras claves. Educación, residencia, postgrado.
Different studies showed that symptoms have a low accuracy for the diagnosis of gastroesophageal reflux disease (GERD) as compared to pH monitoring.1, 2 An objective evaluation of patients with GERD symptoms brings better outcomes after treatment3 and lower costs.4 pHmonitoring allows not only an objective testing for pathologic gastroesophageal reflux but also evaluates temporal correlation between symptoms and episodes of reflux. This temporal correlation also correlates with outcomes.5 The number of symptoms experienced in 24 hours may also represent indirectly hypersensitivity, hypervigilance and psychosocial characteristics that may justify GERD symptoms in patients with a normal pHmonitoring.
This study aims is to correlate the number of symptoms reported during 24-hour pH monitoring with the objective diagnosis of GERD.
Material and methods
Population
We studied 424 non-selected consecutive patients (58% females, median age 41 years, range: 18-77), that underwent ambulatory pH monitoring for suspected GERD. Patients with previous foregut surgery or primary esophageal motility disorders were excluded from the study.
Esophageal function tests
All patients underwent esophageal manometry, to evaluate esophageal motility and to locate the upper border of the lower esophageal sphincter (LES). Medications that interfere with esophageal and gastric motility were discontinued opportunely.
Esophageal pH monitoring was performed in all patients. Acid reducing medications were discontinued 3 (H2 blocking agents) to 10 days (proton pump inhibitors) prior to the study. During the study, the patients consumed an unrestricted diet. The data were incorporated into a composite score (DeMeester score), and a score greater than 14.7 was set as abnormal. Patients were grouped according to abnormal pH monitoring in GERD + or GERD -. The number of symptoms during the test was recorded as well as temporal symptomatic correlation to reflux episodes measured by the symptom index.
Symptoms
Symptoms were grouped in esophageal (heartburn, regurgitation) and extraesophageal (otolaryngologic, pulmonary, thoracic). The most prevalent symptom was considered as the main complaint.
Statistical analysis
Data were presented as mean ± standard deviation. Student’s T, Pearson correlation, Fisher tests and Receiver Operating Characteristic (ROC) curve were used when appropriate. A p value < 0.05 was considered statistically significant.
Ethics
The study protocol was approved by the local Ethics Committee. There are no conflicts of interest. There is no funding. The authors are responsible for the manuscript and no professional writers were hired. Informed consent was waived due to the retrospective format of the study.
Results
GERD + comprised 44% of the total number of patients studied. Demographic data analysis is shown in Table 1. GERD – patients had a higher proportion of females. Symptoms characteristics were not different when groups were compared.
Total number of symptoms, number of esophageal and extraesophageal symptoms, and symptom index were higher in GERD + patients.
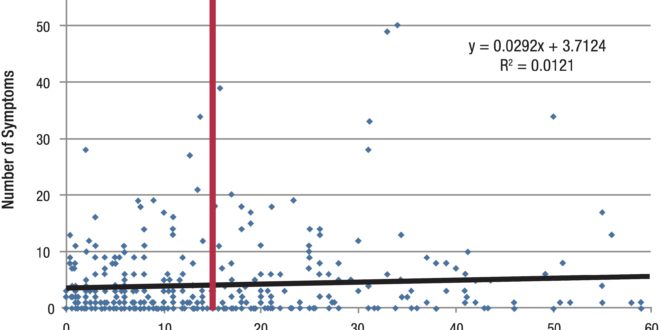
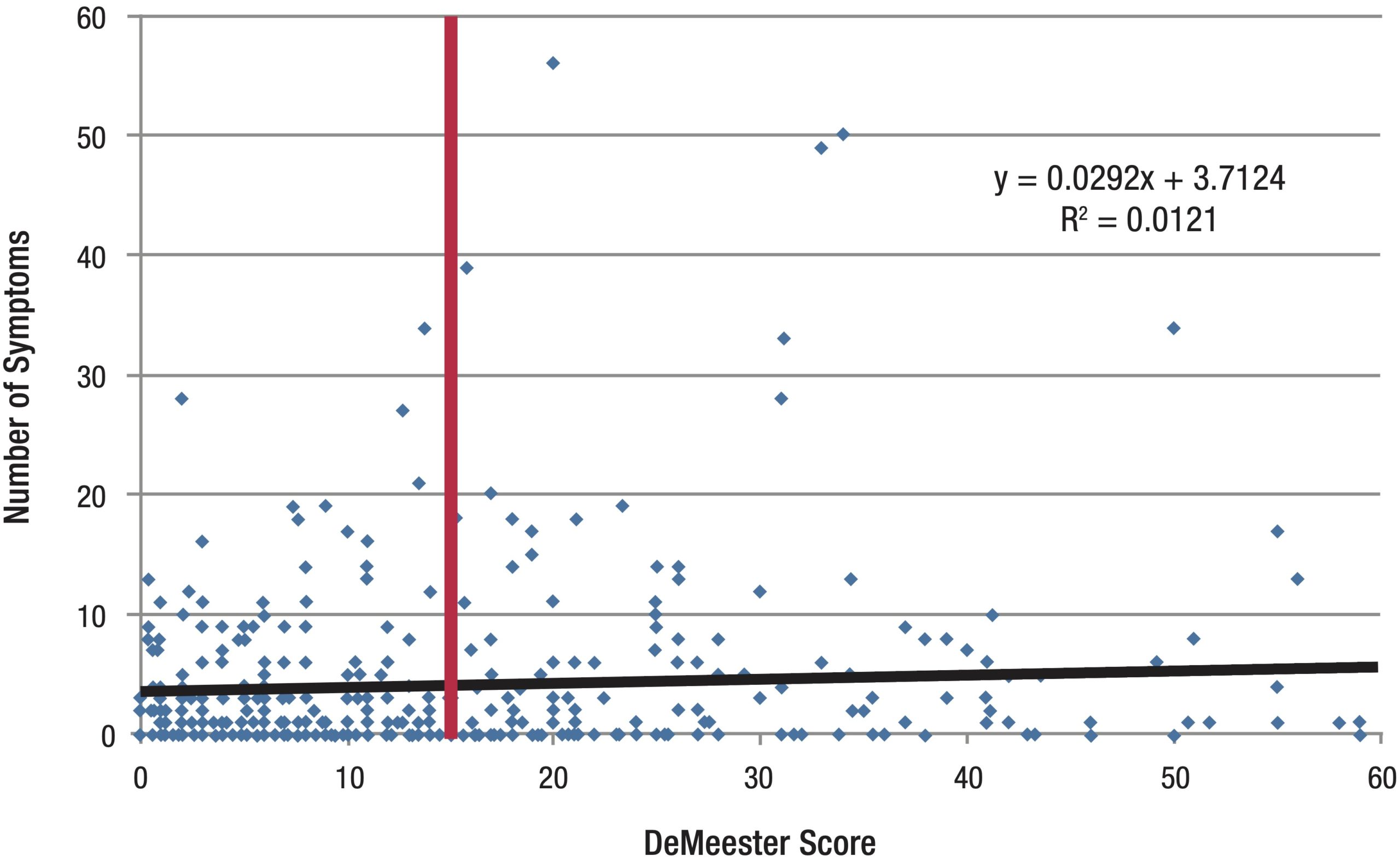
Symptoms and DeMeester score did not correlate for the total number of symptoms (p = 0.8), esophageal symptoms (p = 0.7), extraesophageal symptoms (p= 1.0) and symptom index (p = 0.8) (Figure 1).
Table 1. Patients’ demographics and symptoms according to the presence or absence of gastroesophageal reflux disease (GERD).

Table 2. Number of symptoms reported during pHmonitoring according to the presence or absence of gastroesophageal reflux disease (GERD).

Figure 1. Number of symptoms reported during pHmonitoring according to the presence or absence of gastroesophageal reflux disease (GERD).
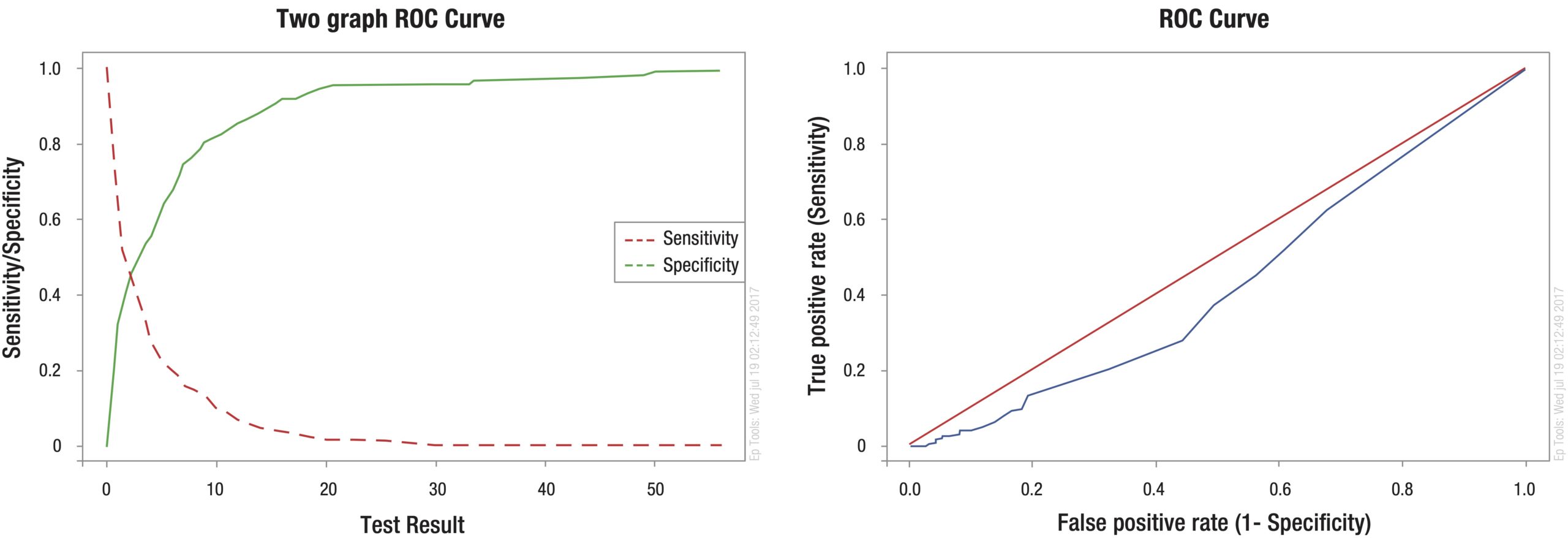
The area under ROC curve was 0.6 for the accuracy of the number of symptoms and the presence of GERD (Figure 2).
Figure 2. Receiver Operating Characteristic (ROC) curve for the accuracy of the number of symptoms and the presence of gastroesophageal reflux disease.
Discussion
It has been shown that symptoms are inaccurate for the diagnosis of GERD. The accuracy for heartburn + regurgitation to diagnose GERD is only 58%, with worse results for extraesophageal symptoms.6 Our results show that less than half of the patients from a population with clinical diagnosis of GERD referred for pHmonitoring actually had GERD. The absence of GERD in patients with extraesophageal reflux symptoms can be explained by the overlap of clinical presentation with pulmonary, otolaryngologic and cardiac diseases.7 Interestingly, however, the same proportion of esophageal and extraesophageal symptoms were found in both patients GERD + and GERD – in our series. Esophageal complaints in GERD – patients may also be caused by dysmotility, visceral hypersensitivity, hypervigilance and psychosocial characteristics.8, 9
The number of symptoms experienced during 24 hours may indirectly represent visceral hypersensitivity, hypervigilance and psychosocial characteristics. We expected a two-tailed distribution of symptoms. We believed that patients who reported a small number of symptoms during pHmonitoring had a lower chance to have GERD, since the disease presents with burdensome symptoms leading to a low quality of life comparable to diabetes and hypertension especially considering that patients had to stop medication to undergo the test.10 Our results oppositely showed a higher number of symptoms in GERD + patients, even though, this parameter is a very weak predictor for GERD. We expected also a higher incidence of total absence of symptoms during pHmonitoring in GERD – patients considering that it is linked to worse outcomes after surgical therapy.5, 11 Our results; however, did not confirm this hypothesis with a likelihood ratio of only 1.1 to not experience symptoms during pHmonitoring in GERD – patients. On the other side, we theorized that hypersensitivity, hypervigilance and psychiatric disorders would bring a higher number of symptoms during the test in GERD – patients. Again, our results; however, showed a higher number of symptoms in GERD + patients. Hypersensitivity occur in patients with symptoms triggered by reflux events despite normal acid exposure.12 Since the number of brief episodes of reflux in a day is higher, even in healthy individuals, would lead to an increased number of symptoms reported.13 We found only 10 patients that could have this diagnosis (4% of GERD – patients). This small number renders difficult any mathematical analysis; however, they reported an average of 10 symptoms during the test, i.e., well above the average for the population. Hypervigilance and psychiatric disorders could also lead to an increased number of daily symptoms since psychological factors affect how patients perceive the physiological symptoms.14 While, some authors showed that the likelihood of complaining of reflux symptoms increased by 2.8 times when anxiety and depression are present,15 others showed that levels of anxiety or depression were not associated with the number of reflux symptoms reported during 24-hour pH impedance monitoring or with the number of symptoms associated with a reflux event.16
In conclusion, our results show that GERD + patients reported higher number of symptoms during pHmonitoring but the number of symptoms is not a good predictor for GERD presence or severity. pH monitoring is essential to evaluate patients with suspected GERD.
Author’s contribution
JRK: acquisition of data, analysis and interpretation of data, drafting the article.
FAMH: acquisition of data, analysis and interpretation of data, drafting the article, final approval of the version to be published.
FML: acquisition of data, analysis and interpretation of data, final approval of the version to be published.
FS: analysis and interpretation of data, final approval of the version to be published.
MP: review for intellectual content, analysis and interpretation of data, final approval of the version to be published.
Meeting presentation. Poster presentation at the 47th World Congress of Surgery, Basel, August 2017.
Conflict of interest. No conflict of interest.
Financial support. Without financial support.
Referencias
- Andolfi C, Bonavina L, Kavitt RT, Konda VJ, Asti E, Patti MG. Importance of Esophageal Manometry and pH Monitoring in the Evaluation of Patients with Refractory Gastroesophageal Reflux Disease: A Multicenter Study. J Laparoendosc Adv Surg Tech A 2016; 26: 548-550.
- Herbella FA, Andolfi C, Vigneswaran Y, Patti MG, Pinna BR. Importance of esophageal manometry and pH monitoring for the evaluation of otorhinolaryngologic (ENT) manifestations of GERD. A multicenter study. J Gastrointest Surg 2016; 20: 1673-1678.
- Andolfi C, Vigneswaran Y, Kavitt RT, Herbella FA, Patti MG. Laparoscopic Antireflux Surgery: Importance of Patient’s Selection and Preoperative Workup. J Laparoendosc Adv Surg Tech A 2017; 27: 101-105.
- Kleiman DA, Beninato T, Bosworth BP, Brunaud L, Ciecierega T, Crawford CV Jr, Turner BG, Fahey TJ 3rd, Zarnegar R. Early referral for esophageal pH monitoring is more cost-effective than prolonged empiric trials of proton-pump inhibitors for suspected gastroesophageal reflux disease. J Gastrointest Surg 2014; 18: 26-33.
- Patti MG, Arcerito M, Tamburini A, Diener U, Feo CV, Safadi B, Fisichella P, Way LW. Effect of laparoscopic fundoplication on gastroesophageal reflux disease-induced respiratory symptoms. J Gastrointest Surg 2000; 4: 143-149.
- Bello B, Zoccali M, Gullo R, Allaix ME, Herbella FA, Gasparaitis A, Patti MG. Gastroesophageal reflux disease and antireflux surgery-what is the proper preoperative work-up? J Gastrointest Surg 2013; 17: 14-20.
- Hom C, Vaezi MF. Extra-esophageal manifestations of gastroesophageal reflux disease: diagnosis and treatment. Drugs 2013; 73: 1281-1295.
- Roman S, Keefer L, Imam H, Korrapati P, Mogni B, Eident K, Friesen L, Kahrilas PJ, Martinovich Z, Pandolfino JE. Majority of symptoms in esophageal reflux PPI non-responders are not related to reflux. Neurogastroenterol Motil 2015; 27: 1667-1674.
- Hsu CS, Wen SH, Hung JS, Liu TT, Yi CH, Lei WY, Pace F, Chen CL. Overlap of Dyspepsia in Patients with Gastroesophageal Reflux Disease: Impact of Clinical, Metabolic, and Psychosocial Characteristics. Dig Dis Sci 2017; 62: 994-1001.
- Revicki DA, Wood M, Maton PN, Sorensen S. The impact of gastroesophageal reflux disease on health-related quality of life. Am J Med 1998; 104: 252-258.
- Chin KF, Myers JC, Jamieson GG, Devitt PG. Symptoms experienced during 24h pH monitoring and their relationship to outcome after laparoscopic total fundoplication. Dis Esophagus 2008; 21: 445-451.
- Aziz Q, Fass R, Gyawali CP, Miwa H, Pandolfino JE, Zerbib F. Functional Esophageal Disorders. Gastroenterology 2016; 150: 1368-1379.
- Neto SC, Herbella FA, Silva LC, Patti MG. Ratio between proximal/distal gastroesophageal reflux does not discriminate abnormal proximal reflux. World J Surg 2014; 38: 890-896.
- Oh JH, Kim TS, Choi MG, Lee H, Jeon EJ, Choi SW, Lee C, Chung IS. Relationship between Psychological Factors and Quality of Life in Subtypes of Gastroesophageal Reflux Disease. Gut Liver 2009; 3: 259-265.
- Jansson C, Nordenstedt H, Wallander MA, Johansson S, Johnsen R, Hveem K, Lagergren J. Severe gastro-oesophageal reflux symptoms in relation to anxiety, depression and coping in a population-based study. Aliment Pharmacol Ther 2007; 26: 683-691.
- Kessing BF, Bredenoord AJ, Saleh CM, Smout AJ. Effects of anxiety and depression in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2015; 13: 1089-1095.
Correspondencia: Fernando Herbella
Rua Diogo de Faria 1087, cj 301. São Paulo- SP 04037-003 Brazil
Tel./fax: 55-11-39267610
Correo electrónico: herbella.dcir@epm.br
Acta Gastroenterol Latinoam 2019;49(4):331-335
