Sharadendu Bali, Rikki Singal
Department of Surgery, Maharishi Markandeshwer Institute of Medical Sciences and Research. Mullana, Distt-Ambala, Haryana, India.
Acta Gastroenterol Latinoam 2018;48(1):35-40
Recibido: 02/03/2017 / Aprobado: 21/06/2017 / Publicado en www.actagastro.org el 19/03/2018

Summary
Even though laparoscopic cholecystectomy emerged over 20 years ago, controversies persist with regards to the best method to ligate the cystic duct and artery. We proposed to assess the safety, cost effectiveness and feasibility of different methods to close the cystic duct and artery by suture ligation versus clip application working in rural area where latest facilities are limited. Even today the latest Harmonic Scalpel and Plasma Kinetic have become popular with the promise of quick and effective vascular control, but again these are less cost-effective and problem of availability in rural area still exists. Aim. Evaluate the effectiveness in terms of cost, safety and complications in ligation of the cystic artery and duct separately with non-absorbable suture ligation compared to clip application. Our aim is for surgeons sitting in rural area, where latest facilities are not available, they can ligate the CD or artery using non-absorbable suture which is cheaper and cost-effective without encountering any bile leakage or bleeding. Silk suture can be tied near to the CBD as risk of involving the CBD wall is less as compared to clips. Settings and design. A prospective randomised double blind study. Material and methods. This was a randomised controlled prospective study carried out at a medical college hospital (in remote village) from period of January 2011 to February 2012 in India. A total number of 160 cases were selected in the study, out of which 40 cases were excluded as per the selection criteria. Patients were selected randomly and divided into two groups diagnosed as chronic cholecystitis (cholelithiasis). In group A (study group-60 cases) cystic pedicle was ligated by silk sutures 2-0 (intracorporeal knots) while in group B (control group-60 cases) cystic pedicle was closed with titanium clips using a clip applicator. Results. Out of total 120 patients, in group A (60 patients), cystic duct and artery were ligated separately using silk suture and in group B (60 patients) the pedicle was closed using titanium clips. The operative time in group A was 30 to 50 mins and in group B it was 30 to 40 minutes (p = 0.015). The time required for suture ligation was 6.5 ± 1.3 mins and for ligaclips it was only 4 ± 1.1mins thus decreasing the overall operative time of the procedure (p > 0.001). Drainage was required in 45 patients in A and in 40 patients in group B. It was removed on 2nd of surgery according to the colour and volume. Overall cost of procedure was more in group B as compared to group A. There was no statistically significant difference found between the two groups in terms of length of inpatient stay, post-operative complications and safety of procedure. However, the mean operative time was lesser in whom cystic artery and duct were clipped than suture ligation. Conclusion. The ligation with suture needs more expertise than clip which is easy for trainees. It is difficult where latest and well equipped centres are there for cystic pedicles. If facilities for multiple clip sizes are not available, then silk ligature is the other option and cost-effective, especially in rural centres.
Key words. Laparoscopic cholecystectomy, intracorporeal ligation, clips, complications, cystic duct leaks.
Sutura laparoscópica versus la colocación de clips en la colecistectomía: consejos y estrategias para mejorar la eficacia y la seguridad
Resumen
A pesar de que la colecistectomía laparoscópica surgió hace más de 20 años, las controversias persisten con respecto al mejor método para ligar el conducto y la arteria cística. Nos propusimos evaluar la seguridad, la rentabilidad y la viabilidad de diferentes métodos para cerrar el conducto y la arteria cística por ligadura de sutura versus la aplicación de clips en quienes trabajan en áreas rurales donde los recursos son limitados. Incluso hoy en día el último bisturí armónico y plasma cinética se han popularizado, con la promesa de realizar un control vascular rápido y eficaz, pero son menos rentables y el problema de su disponibilidad en el área rural todavía existe. Objetivo. Evaluar la eficacia en términos de costo, seguridad y complicaciones de la ligadura del conducto y la arteria cística por separado con ligadura de sutura no absorbible en comparación con la aplicación de un clip. Nuestro objetivo es que los cirujanos que trabajan en área rural, donde las instalaciones más modernas no están disponibles, puedan utilizar suturas para ligar el conducto cístico o la arteria. Incluso la sutura no reabsorbible es más económica y de larga duración, sin que se produzca ninguna fuga de bilis o sangrado. La sutura de seda se puede unir cerca del conducto biliar común ya que no involucra la pared del mismo en comparación con los clips, pero se debe asegurar que sea técnicamente lo suficientemente adecuada para que no se produzcan fugas ni sangrados. Diseño. Estudio prospectivo, aleatorizado y doble ciego. Material y métodos. El estudio fue desarrollado en el hospital universitario de medicina (en aldea remota) en la India, desde enero de 2011 hasta febrero de 2012. Ingresaron al estudio un total de 160 casos, de los cuales fueron excluidos 40, según los criterios de selección. Los pacientes fueron seleccionados aleatoriamente y divididos en dos grupos, con diagnóstico de colecistitis crónica (colelitiasis). En el grupo A (grupo de estudio – 60 casos), el pedículo cístico se ligó mediante suturas de seda 2-0 (nódulos intracorpóreos) mientras que en el grupo B (grupo de control – 60 casos) el pedículo cístico se cerró con clips de titanio utilizando un aplicador de pinzas. Resultados. De un total de 120 pacientes, en el grupo A (60 pacientes), el conducto cístico y la arteria se ligaron por separado utilizando sutura de seda, y en el grupo B (60 pacientes) se cerró el pedículo con clips de titanio. El tiempo operativo en el grupo A fue de 30 a 50 minutos y en el grupo B fue de 30 a 40 minutos (p = 0,015). El tiempo requerido para la ligadura de la sutura fue de 6,5 ± 1,3 minutos y para los ligaclips fue de solo 4 ± 1,1 minutos, disminuyendo así el tiempo operativo general del procedimiento (p > 0,001). Se requirió drenaje en 45 pacientes del grupo A y en 40 pacientes del grupo B. Se retiraron después de la cirugía según el color y el volumen. El costo total del procedimiento fue mayor en el grupo B, en relación con el grupo A. No hubo diferencia estadísticamente significativa entre los dos grupos en cuanto a la duración de la estancia hospitalaria, las complicaciones postoperatorias y la seguridad del procedimiento. Sin embargo, el tiempo medio operatorio fue menor en los casos en los que se cortó la arteria cística y el conducto, comparado con la ligadura de sutura. Conclusión. La ligadura con la sutura necesita más experiencia que el clip, que es más fácil para los practicantes. Si las instalaciones para múltiples tamaños de clip no están disponibles, entonces la ligadura de seda es la otra opción rentable, especialmente en los centros rurales.
Palabras claves. Colecistectomía laparoscópica, ligadura intracorpórea, clips, complicaciones, fugas del canal cístico.
Abreviatures
LC: laparoscopic cholecystectomy.
USG: ultrasonography.
CD: cystic duct.
CBD: common bile duct.
Cholecystectomy is the second most commonly performed intra-abdominal operation worldwide after appendicectomy. It has enjoyed largely an unchallenged supremacy as the treatment of choice in cholelithiasis since it was performed by Carl Langenbuch in 1882. In 1983 Kurt Semm used an automatic insufflation device for assessing the intra-abdominal pressures.1 In standard cholecystectomy, however there is considerable discomfort on the part of the patients in terms of size of incision, wound infection, bleeding and hospital stay. Laparoscopic surgery has become the method of choice for treatment of symptomatic and uncomplicated gallbladder stones, appendectomies and hernia repair.2
Some studies compared the harmonic scalpel and clip to close the cystic duct and cystic artery in a single incision laparoscopic cholecystectomy (LC). They concluded that, there was no conversion to open surgery or need of additional port in any patients and the operative data was the same in both groups. During the follow up period, one port site hernia was developed in patient. Harmonic scalpel has been recently used for ligating cystic pedicle which is feasible, safe and effective performing LC although cost is a constraint.3
Material and methods
The study was carried out in the Department of General Surgery MMIMSR, Mullana, Ambala from January 2011 to February 2012. Information on ethics committee approval and informed consent was taken with project number-IEC/MMIMSR/14170. In this study, a total of 160 cases underwent LC with different techniques for closure of the cystic pedicles out of which 40 cases excluded as per the selection criteria. The cases were randomly allocated by a computer algorithm into the study group A (60 cases) and control group B (60 cases). All cases diagnosed as chronic cholecystitis with cholelithiasis were included in the study. Patients were diagnosed with perforated gallbladder, empyema gallbladder, common bile duct stones, acute abdomen, bleeding disorders, pregnancy and those patients not fit for surgery were excluded. All patients will undergo routine blood tests in view of cholelithiasis including ultrasonography (USG) abdomen and chest X ray. All patients were given routine pre-operative (60 min before operation) and post-operative antibiotics (ceftriaxone 1 g, amikacin 500 mg, metronidazol 500 mg). Surgery performed under general anaesthesia and patient kept in the supine position with 30-degree head up and right lateral side elevated. The surgeon and the camera assistant stood on the left side of the patient. In both groups 4 ports were used, 10 mm for infraumblical, epigastrium and 5 mm port for other two ports. After dissecting Calot’s triangle, a proper exposure of cystic artery and cystic duct was made.
Cystic duct (CD) exposed distally up to gallbladder and proximally upto the common bile duct. In group A, CD and artery was ligated with non-absorbable suture silk no-2-0 intracorporeally in a surgeon’s knot configuration, whereas in group B, titanium ligaclips of sizes large and medium were applied for CD and artery respectively. In both groups, CD and artery closed separately. We also emphasize on the technique used for closure of the cystic duct with clip, two clips applied on the proximal part of the CD and one clip used on distal side. If space is less or CD is shorter, in these cases we applied clip obliquely away from the common bile duct. In group A, silk was tie applied and assured that it should not be loose to prevent any leakage. Another advantage of silk is that, it can be tied close to the common bile duct (CBD). Drain will be kept in all the patients in sub hepatic area.
Results
A total number of 120 patients selected randomly and divided into two groups A and B. Patients in whom cystic pedicle was ligated using suture were assigned group A (60 cases), and the one in whom ligaclips were used were named under group B (60 cases). In group A, there were 24 males and 36 females, whereas in group B there were 23 males and 37 females. Both groups had cholelithiasis and acute attack was excluded using history, clinical examination and pre-operative imaging. Patients in whom cystic pedicle was ligated using suture were assigned group A, and the one in whom ligaclips were used were named under group B. The mean operative time in group A was 30 – 50 minutes and in group B it was 30 – 40 minutes (p = 0.015). The time required for suture ligation was 6.5 ± 1.3 min and for ligaclips it was only 4 ± 1.1 min thus decreasing the overall operative time of the procedure (p > 0.001) which was significant. Drain was removed when the volume decreased to < 20 ml/24 hours and colour of the discharge becomes light serous. Only in three cases there was bile in the discharge which remains only for four days. The mean operative time less in whom cystic artery and duct was closed with titanium clips as compared to the silk ligature which was significant. There were no major differences seen in both groups in terms of inpatient stay, post-operative complications and safety of the procedure (Table 1 and 2). Hospital stay in both groups was same i.e. 2 to 3 days. Ryle’s tube was removed in evening on same day of surgery. On next day patient was allowed orally sips of water and by evening full diet and planned for discharge on 2nd day of surgery. In four cases hospital stay was three to four days. The ligation with suture needs more expertise than the clip application. Silk has the more advantageous over the clip, as it will be cost-effective, economical and available freely especially in rural area. So, the surgeon should be well versed with both methods (Figure 1 and 2). All patients observed post-operatively for any fever, wound infection, haemorrhage, any intra-abdominal collection and the length of stay in hospital. There were no major complications seen in both groups. Patients were followed for two weeks and would be inquired about fever, vomiting, scar pain or any collection inside the abdomen. We compared the results of both studies in view of efficacy, safety, complications, cost-effectiveness and hospital stay. In both studies there were no complications seen except for the little prolonged timing in group A as compared to other group.
Tabla 1. Pre-operative parameters.
Tabla 2. Intraoperative parameters and post-operative data.
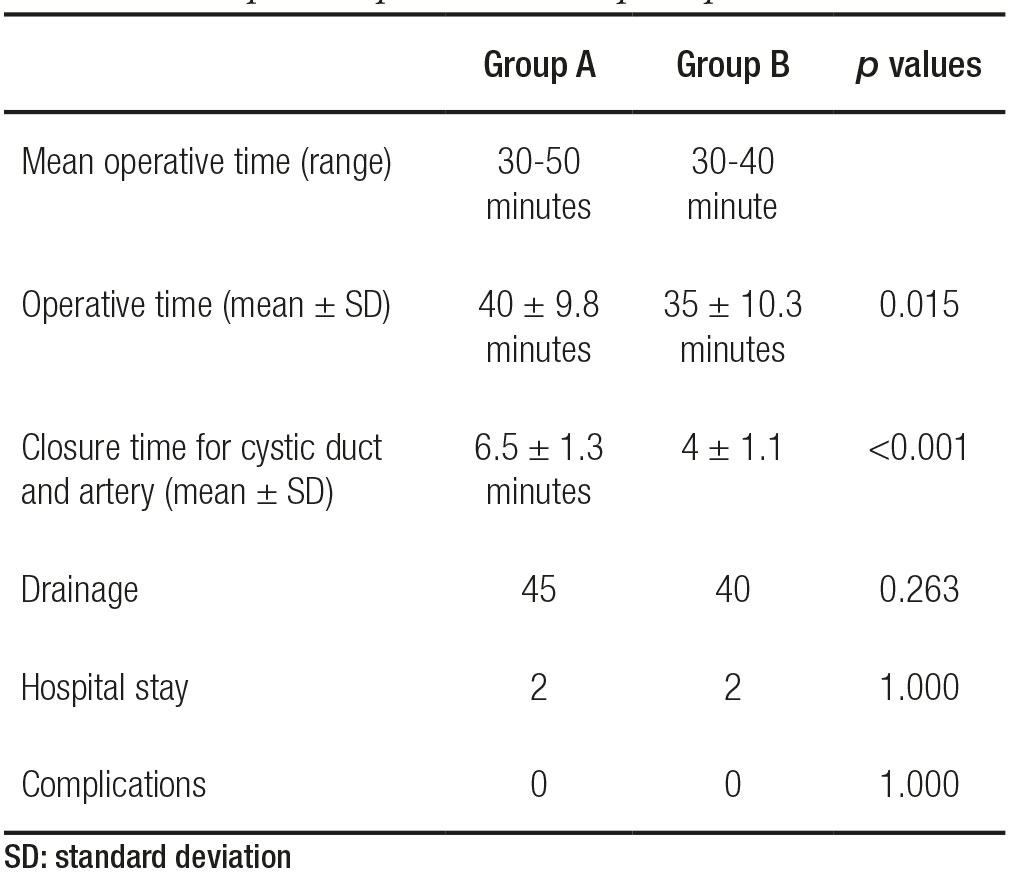
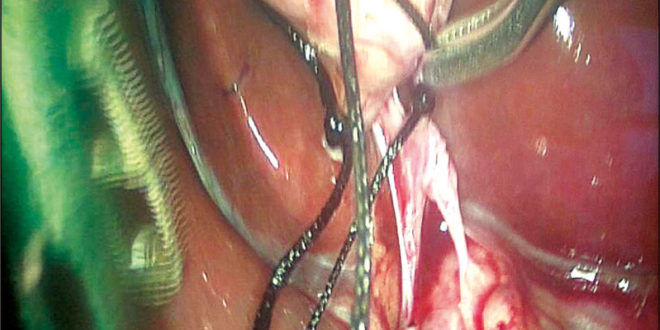
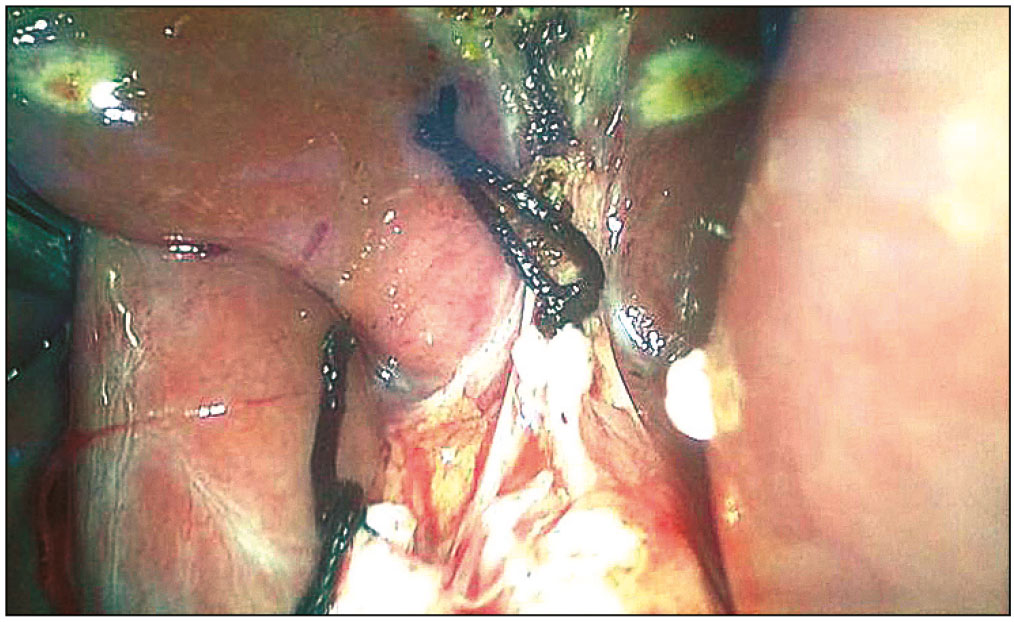
Figure 1. Operative picture showing ligating the cystic duct and artery separately.
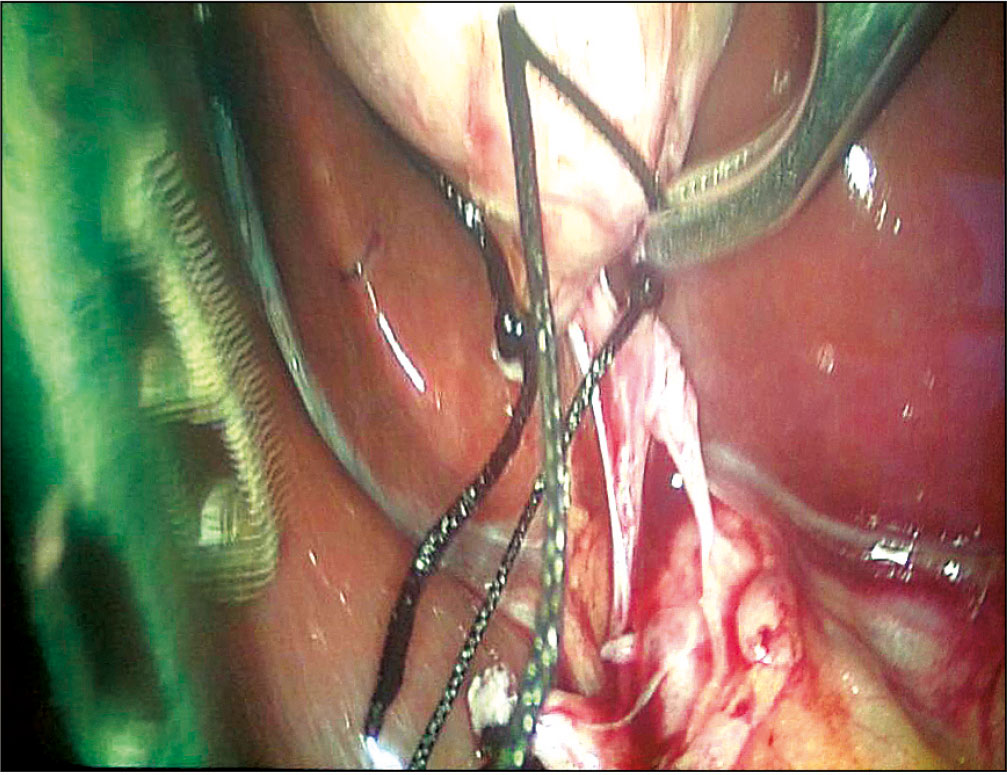
Figure 2. Section revealed two cut parts as cystic duct and artery along with silk tie.
Discussion
Cholelithiasis and its consequences are the main cause of surgical entry into the peritoneal cavity. So widespread is this entity that it will not be out of place to say that cholecystectomy is routinely done.4 The monopolar cautery used to separate the cystic artery and the CD was closed by non-absorbable sutures. They stated that the CD ligation is safe, possible, practical and cost effective. They observed no leakage of bile from CD stumping where the harmonic scalpel was used. Other alternate techniques include linear stapler, endoloops, knots, harmonic scalpels.5 Minimal invasive surgery or key hole surgery has become the method of preference for the treatment of uncomplicated gallbladder stones, hernia repair and appendectomies.6 The two groups were compared between monopolar electro surgery and clips in the form of hospital stay, timing, and complications. Their study observed the harmonic scalpel can be used to shorten the duration of surgery and cost saving that is inherent in a technique using it as a single device.7
Another study stated that harmonic scalpel is useful to control the bleeding. The closure of cystic duct with newer methods may be an alternative to surgical clips.8 The CD and artery are normally closed with titanium clips. They declared no bile leakage or other problems with the intracorporeal ligation of the cystic duct/artery by silk 2/0. The time required for tie was varied from 2-7 minutes.9 Other study formatted four points to increase the safety of the surgery; a) proper site of the trocar, b) identification and proper dissection from the Hartmann’s pouch at first, c) to decrease bile leakage, closer of the CD and cystic artery by intracorporeal suturing is necessary d) the gallbladder can be removed from the umbilical trocar site. It will make feasible, easy for the surgeons to perform surgery that will show better cosmetic.10 Bile leakage from the CD may occur due to improper clip application, perforation proximal to clips, and stump necrosis. They observed that CD leaks commonly seen in LC than open cholecystectomy.11 Others stated that, after cholecystectomy cystic duct leakage is frequently seen. The purpose was to evaluate the bipolar sealing system (ligature) for closure of CD. They declared that in LC, ligature was quick and helpful for closure and separation of cystic duct.12 With adequate identification closure and division of cystic duct/artery with branches remain an integral condition for dissection of the gallbladder.
Various papers emphasize the role of ultrasound dissection in LC, where ultrasonic devices have been applied in removal of the gallbladder. LC is the commonly accepted technique which routinely used with conventional laparoscopic instruments. Some comparable results in between harmonic scalpel versus clip in leakage of bile (cystic duct/common bile duct/accessory duct) 1.75% and 0.66%, respectively. The harmonic scalpel is effective and advantageous over to clip application for closure of the CD.13-15 Others observed that the operative time was 31.5 ± 11.1 minutes in Group B, 33.1 ± 10 minutes in Group A, and 36.5 ± 9.9 in Group C. Their results were statistically significant (p < 0.04) in Group B and Group C. The opening pressure in cystic duct was more (324.0 ± 23.4 mmHg) in Group A. In LC different energy source instruments may be safe to use with a cautious dissection and sealing of the cystic duct.16 The results of the experiment on animal liver tissue showed that the use of harmonic scalpel during gallbladder removal is a safer with much lower risk of complications than the use of ordinary electro cautery. They analysed the impact of coagulation instrument devices used during gallbladder removal.17 In our study the mean operative time in group A was 30 – 50 minutes and in group B it was 30 – 40 minutes (p = 0.015). The time required for suture ligation was 6.5 ± 1.3 min and for ligaclips it was only 4 ± 1.1 min thus decreasing the overall operative time of the procedure (p < 0.001). We observed that silk suture is safe, cost effective but it required training as compared to clip application. But for clip application you required clip applicator which is again costly. There may be chances of slippage of clips or it may cause stricture formation if it involved the wall of the CBD though in our study we have not encountered such complications. At end, the use of ligatures instead of ligaclips for LC, especially the interest in expanding its realization in rural areas with fewer resources.
Conflict of interest. None.
References
- Gupta R, Singal R, Sharda VK, Singh B, Ahluwalia JS, Bhatia G, Arora G. Two port laparoscopic assisted appendicectomy versus three port laparoscopic appendicectomy: A prospective study of 50 cases. Trop J Med Res 2015; 18: 14-19.
- Zaman M, Singal S, Singal R, Shah A, Sandhu KS, Singh B, Khera A, Bassi S. Comparison of open and closed entry techniques for creation of pneumoperitoneum in laparoscopic surgery in terms of time consumption, entry related complications and failure of technique. World J Lap Surg 2015; 8: 69-71.
- Huseyin Y, Husnu A, Ilhan E, Akın C, Mustafa S. Closure of the Cystic Duct: Comparison to harmonic scalpel versus clip application in single incision laparoscopic cholecystectomy. J Gastroint Dig Syst 2014; 4: 165.
- Singal R, Singal RP, Sandhu K, Singh B, Bhatia G, Khatri A, Sharma BP. Evaluation and comparison of postoperative levels of serum bilirubin, serum transaminases and alkaline phosphatase in laparoscopic cholecystectomy versus open cholecystectomy. J Gastrointest Oncol 2015; 6: 479-486.
- El-Geidie AA. Single-incision laparoscopic cholecystectomy (SILC) using harmonic scalpel. J Surg Res 2012; 176: 50-54.
- Singal R, Zaman M, Mittal A, Singal S, Sandhu K, Mittal A. No need of fascia closure to reduce trocar site hernia rate in laparoscopic surgery: a prospective study of 200 non-obese patients. Gastroenterology Research 2016; 9: 70-73.
- Gelmini R, Franzoni C, Zona S, Andreotti A, Saviano M. Laparoscopic cholecystectomy with harmonic scalpel. JSLS 2010; 14: 14-19.
- Tahir Ozer M, SinanH, Kilbas Z, Kagan Coskun A, Gunal A, Demirbas S, Kantarcioglu M, Ihsan Uzar A, Kozak O. Comparison of different cystic duct closure methods in laparoscopic cholecystectomy: silk suture, surgical clip, harmonic scalpel and plasma kinetic. Arch Clin Exp Surg 2012; 1: 168-171.
- Shah JN, Maharjan SB. Clipless laparoscopic cholecystectomy – a prospective observational study. Nepal Med Coll J 2010; 12: 69-71.
- Talebpour M, Panahi M. New aspects in laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech A 2007; 17: 290-295.
- Woods MS, Traversp LW, Kozarek RA, Tsao J, Rossi RL, Gough D, Donohue JH. Characteristics of biliary tract complications during laparoscopic cholecystectomy: a multi-institutional study. Am J Surg 1994; 167: 27-33.
- Schulze S, Damgaard B, Jørgensen LN, Larsen SS, Kristiansen VB. Cystic duct closure by sealing with bipolar electrocoagulation. JSLS 2010; 14: 20-22.
- Torres K, Chrościcki A, Golonka A, Torres A, Staśkiewicz G, Palczak R, Ceja-Sánchez JM, Ceccaroni M, Drop A. The course of the cystic artery during laparoscopic cholecystectomy. Folia Morphol (Warsz) 2009; 68: 140-143.
- Oruc MT, Ugurlu MU, Boyacioglu Z. Transumbilical multiple-port laparoscopic cholecystectomy using standard laparoscopic instruments. Minim Invasive Ther Allied Technol 2012; 21: 423-428.
- Wills E, Crawford G. Clipless versus conventional laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech A 2013; 23: 237-239.
- Bulus H, Basar O, Tas A, Yavuz A, Akkoca M, Coskun A, Coban S, Tuna Y, Erbis H, Koklu S. Evaluation of three instruments for laparoscopic cholecystectomy: harmonic scalpel, bipolar vessel sealer, and conventional technique. Minerva Chir 2013; 68: 537-542.
- Hasala P. Rates of complications after laparoscopic cholecystectomy depending on the coagulation technique – a comparative study. Rozhl Chir 2012; 91: 158-163.
Corresponding: Sharadendu Bali
Department of Surgery, Maharishi Markandeshwer Institute of Medical Sciences and Research. Mullana, Distt-Ambala (Pin!-Code: 133203), Haryana, India. Tel. (Cel.): 7838919500 /Fax: 01731304550
Correo electrónico: drsharadbali@yahoo.com
Acta Gastroenterol Latinoam 2018;48(1): 35-40
