Sayantan Bhattacharya
Consultant Surgeon, Warrington Hospital. Lovely Lane, Warrington, Cheshire, England.
Acta Gastroenterol Latinoam 2018;48(1):41-43
Recibido: 07/11/2017 / Aprobado: 18/12/2017 / Publicado en www.actagastro.org el 19/03/2018

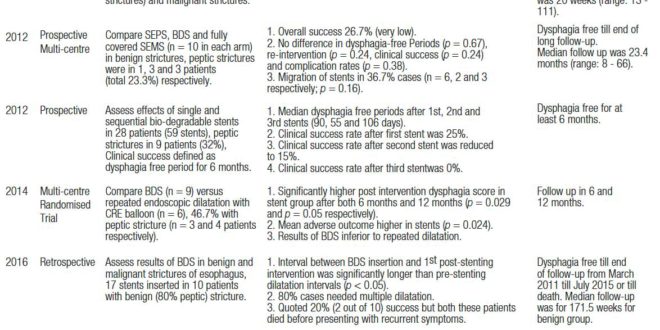
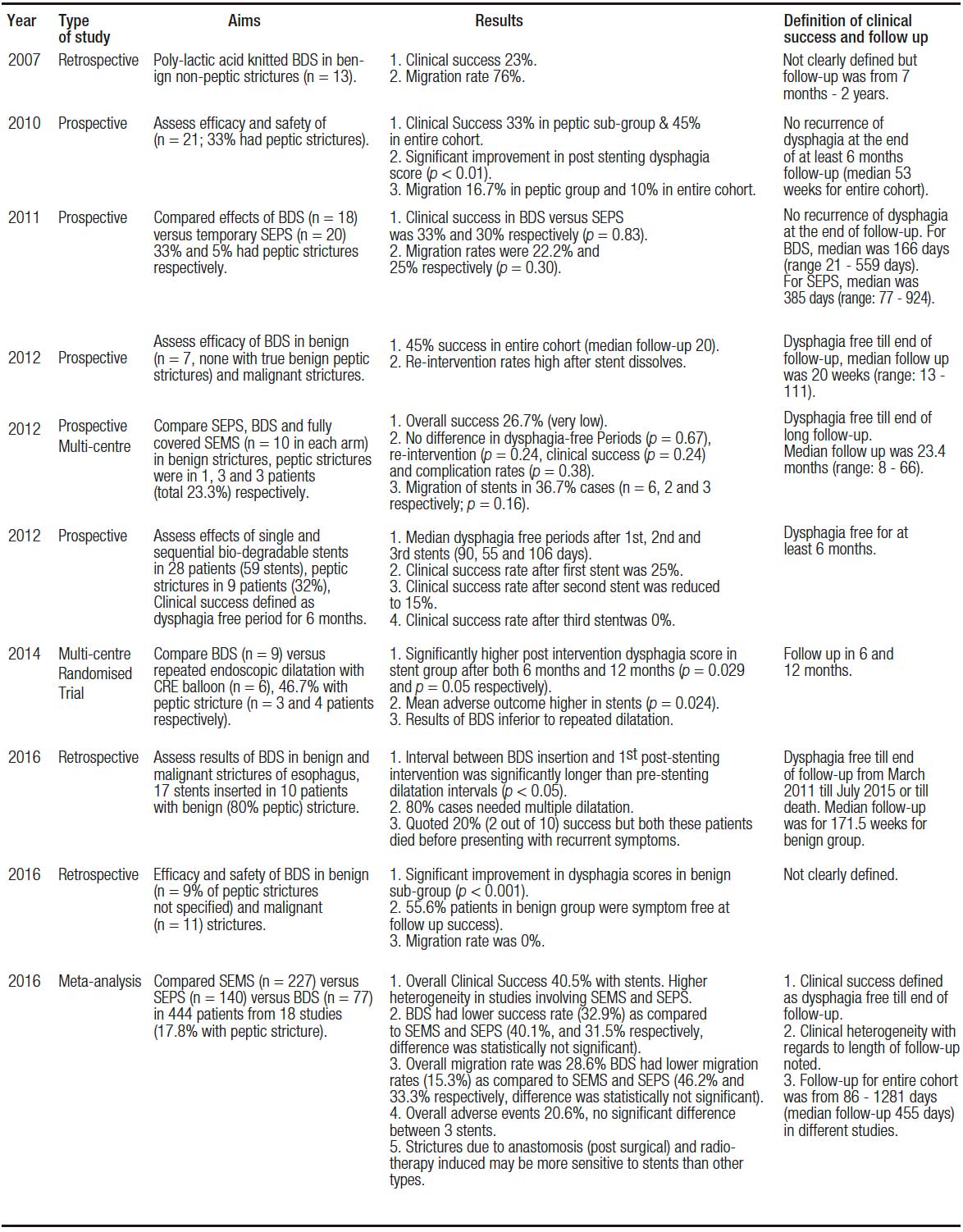
Treating resistant peptic oesophageal strictures still poses significant challenge to gastroenterologists and GI surgeons around the globe. Although traditional treatment is repeated endoscopic dilatation, there is no clear evidence regarding their indicated frequency or degree of stretching, required for achieving best results. Patients are mostly in their extremis and malnourished, prone to complications from factors both related and unrelated to interventions. Hence, any possible alternative which reduces number of invasive interventions or increases their intervals are worth exploring. In quest for this, use of steroid injection with endoscopic stretching and stents of different varieties have been investigated. Endoscopic steroid injection to the stricture site was reported initially as a better option over endoscopic dilatation alone, however, in absence of a specified dose of injection, set regime and added risk of delayed perforation is still under review.1 After several initial reports of complications and low success rates in benign setting with metal and plastic stents (embedding, migration and need for re-intervention), biodegradable stents (BDS) emerged as a more viable alternative. However, studies failed to show success rates of more than 55% with BDS. Most of these studies were prospective or retrospective models, with small cohort size.2-5 Most studies used heterogeneous cohorts comprising of strictures from several aetiologies, thus introducing selection bias, as a recent meta-analysis found association between aetiology and treatment outcome in benign strictures.6 Different follow-up periods were used to define clinical success in most studies. Hence, inferences drawn regarding success rates were comparable between reports with difficulty. A randomised trial reported inferior performance of BDS with respect to mean number of adverse outcomes, post intervention dysphagia-score at 6 and 12 months as compared to endoscopic dilatation alone, in benign setting (Table 1).7 This was also in clear contradiction to reports from non-randomised studies claiming superiority of BDS in providing greater dysphasia free intervals.8 The meta-analysis, after analysing results from 444 patients and 18 studies, reported no significant difference between results from plastic or metal stents and BDS in benign strictures.6 The authors, however, warned about high levels of heterogeneity in participant studies, especially those involving plastic and metal stents. There was also the obvious risk of amplification of bias from several participant studies which were largely non-randomised.
Lastly, stents are liable to cause more strictures at its ends for reasons not entirely clear to us.9 Probably by keeping the gastro-oesophageal junction open at all times, stents promote continued reflux which is the likely contributory factor. This may also be a reason for shorter dysphagia free intervals with sequential stenting in recurrent stricture.10
Hence, prior to advocating its routine use in benign conditions and replacing current treatment with regular endoscopic dilatations with stents, further targeted studies with larger, non-heterogeneous cohorts, longer follow-up periods and more robust evidence base is required.
Table 1.
References
- Kochhar R, Makharia GK. Usefulness of intralesional triamcinolone in treatment of benign esophageal strictures. Gastrointestinal Endoscopy 2002; 56: 829-834.
- Saito Y, Tanaka T, Andoh A, Minematsu H, Hata K, Tsujikawa T, Nitta N, Murata K, Fujiyama Y. Usefulness of biodegradable stents constructed of poly-l-lactic acid monofilaments in patients with benign esophageal stenosis. World J Gastroenterol 2007; 13: 3977-3980.
- van Boeckel PG, Vleggaar FP, Siersema PD. A comparison of temporary self-expanding plastic and biodegradable stents for refractory benign oesophageal strictures. Clinical Gastroenterology and Hepatology 2011; 9: 653-659.
- McCain S, Quinn B, Gray R, Morton J, Rice P. The role of biodegradable stents in the management of benign and malignant esophageal strictures: a cohort study. The Surgeon. Journal of the Royal Colleges of Surgeons of Edinburgh and Ireland 2016; 14: 322-326.
- Canena JM, Liberato MJ, Rio-Tinto RA, Pinto-Marques PM, Romão CM, Coutinho AV, Neves BA, Santos-Silva MF. A comparison of the temporary placement of 3 different self-expanding stents for the treatment of refractory benign esophageal strictures: a prospective multicentre study. BMC Gastroenterol 2012; 12: 70.
- Fuccio L, Hassan C, Frazzoni L, Miglio R, Repici A. Clinical outcomes following stent placement in refractory benign esophageal stricture: a systematic review and meta-analysis. Endoscopy 2016; 48: 141-148.
- Dhar A, Close H, Viswanath YK, Rees CJ, Hancock HC, Dwarakanath AD, Maier HR, Wilson D, Mason MJ. Biodegradable stent or balloon dilatation for benign esophageal stricture: pilot randomised controlled trial. World J Gastroenterol 2014; 20: 18199- 18206.
- Sigounas DE, Siddhi S, Plevris JN. Biodegradable esophageal stents in benign and malignant strictures – a single center experience. Endosc Int Open 2016; 4: E618-E623.
- Baron TH. Management of benign esophageal strictures. Gastroenterol Hepatol 2011; 7: 46-49.
- Hirdes MM, Siersema PD, van Boeckel PG, Vleggaar FP. Single and sequential biodegradable stent placement for refractory benign esophageal strictures: a prospective follow-up study. Endoscopy 2012; 44: 649-654.
Correspondencia: Sayantan Bhattacharya
Warrington Hospital. Lovely Lane, Warrington, (WA51QG) Cheshire, England
Correo electrónico: sayan.bhattacharya@whh.nhs.uk
Acta Gastroenterol Latinoam 2018;48(1): 41-43
