Francisco Tustumi, Rodrigo Hideki Uema, Flavio Roberto Takeda, Guilherme Luiz Stelko Pereira, Rafaela Brito Bezerra Pinheiro, Rubens Antonio Aissar Sallum, Ulysses Ribeiro Junior, Ivan Cecconello
Instituto do Cancer do Estado de Sao Paulo (ICESP). Brazil.
Acta Gastroenterol Latinoam 2017;47(2):122-125
Recibido: 11/07/2016 / Aprobado: 27/12/2016 / Publicado en www.actagastro.org el 03/07/2017

Summary
The two main histologic esophageal cancer subtypes are squamous cell carcinoma and adenocarcinoma. Other subtypes are uncommon and consequently poorly studied. Esophageal carcinosarcoma is a rare neoplasm, accounting for about 1% of all esophageal tumors. It is a mixed neoplasm, composed by both carcinoma and sarcomatous components. The present study aims to investigate clinical and pathological features of esophageal carcinosarcoma patients followed in a single oncologic center. A retrospective analysis and review of literature of esophageal carcinosarcoma was performed. Diagnosis of this tumor was based on immunohistochemistry. Among 1.574 patients with esophageal malignancies, six (0.38%) were diagnosed with carcinosarcoma (one woman and five men). Mean age was 63.2 (range 53-76) years old. All cases presented a mixed tumor with squamous cell carcinoma. Two patients were submitted to curative intent surgery. Half patients presented metastasis at diagnosis. One patient is still alive at the present moment, and 3 patients died with less than 2 years of follow-up. Esophageal carcinosarcoma is a rare poorly studied tumor. Some case series suggest these neoplasms have low invasiveness rate, and low rate of nodal dissemination, leading to a better prognosis than other esophageal cancer. These statements are not supported by our study. Most of the patients had bad prognosis, with advanced stages tumors at diagnosis and low overall survival.
Key words. Esophageal neoplasms, carcinosarcoma, rare diseases.
Carcinosarcoma esofágico. Experiencia institucional y revisión de la literatura de esta rara enfermedad
Resumen
Los dos principales subtipos histológicos de cáncer de esófago son el carcinoma de células escamosas y el adenocarcinoma. Otros subtipos son poco frecuentes y por consiguiente poco estudiados. El carcinosarcoma de esófago es una neoplasia rara, que representa aproximadamenteel 1% de todos los tumores del esófago. Es un tumor mixto, compuesto por dos componentes, carcinoma y sarcoma. El presente estudio tiene como objetivo investigar las características clínicas y patológicas de los pacientes con carcinosarcoma esofágico seguidos en un único centro oncológico. Se realizó un análisis retrospectivo y la revisión de la literatura de carcinosarcoma de esófago. El diagnóstico de este tumor se basó en la inmunohistoquímica. Entre 1.574 pacientes con neoplasias esofágicas, seis (0,38%) fueron diagnosticados como carcinosarcoma (una mujer y cinco hombres). La edad mediana fue de 63 años (rango: 53-76). Todos los pacientes presentaron un tumor mixto con carcinoma de células escamosas. Dos pacientes fueron sometidos a cirugía con intención curativa. La mitad de los pacientes presentaron metástasis al momento del diagnóstico. Un paciente está vivo en el momento actual, 3 pacientes fallecieron con menos de 2 años de seguimiento. Algunas series de casos sugieren que estos tumores son de baja invasividad y baja tasa de diseminación linfática, lo que haría a un mejor pronóstico que otros cánceres esofágicos. Estas afirmaciones no son compatibles con nuestro estudio. La mayoría de los pacientes tenían mal pronóstico, con tumores en estadios avanzados al momento del diagnóstico y baja tasa de supervivencia.
Palabras claves. Neoplasia esofágica, carcinosarcoma, carcinoma.
Abbreviations
SCC: squamous cell carcinoma.
PC: paclitaxel and carboplatin.
PT: cisplatin and paclitaxel.
IP: irinotecan and cisplatin.
CK: cytokeratin.
Carcinosarcoma, also known as sarcomatoid carcinoma, spindle cell carcinoma, or pseudosarcoma is a rare disorder that can affect various organs, mainly uterus and female reproductive system.1 It is a mixed type of neoplasm, with coexisting epithelial and mesenchymal components.2
Carcinosarcoma accounts for only 0.32-2.4% of esophageal malignancies.3-6 Due to its rarity, little is known about this entity. Esophageal carcinosarcoma is believed to have a better prognosis than other esophageal cancer types, although this statement is controversial. It is believed that esophageal carcinosarcoma usually have low nodal spread rate and low invasiveness rate, with polypoid and intraluminal growth, what would lead to early symptoms.7, 8
The present study is a descriptive report on clinical and pathological features of esophageal carcinosarcoma cases in a single oncologic center along 8 years of experience, and a review of the literature.
Patients and methods
All esophageal cancer patients’ charts of our institution were reviewed, between 2008 and 2016. Cases of sarcomatoid neoplasm were identified and clinical and pathological features of these patients were assessed. For carcinosarcoma diagnosis, cases were submitted to immunohistochemistry. Carcinosarcoma components were identified by cytokeratin detection (CK-5/6, AE-1/AE-3, 35BH11 or 34BE12) or tumor protein p63, and sarcomatous elements were identified by vimentin detection. This project was approved by local institutional ethics committee.
Results
A total of 1.574 of esophageal cancers was reviewed. Six (0.38%) cases of carcinosarcoma were selected, 1 female and 5 male patients (Table 1). Median age was 63 (range:53-76) years old.
Of these patients, 2/6 had previous history of high amount of alcohol intake and all were tobacco smokers. One of these cases was previously diagnosed with Chagasic megaesophagus (Patient “2”).
Tumors had vegetating endoscopic features. Patient «2» had a pediculated aspect, with intraluminal growth.
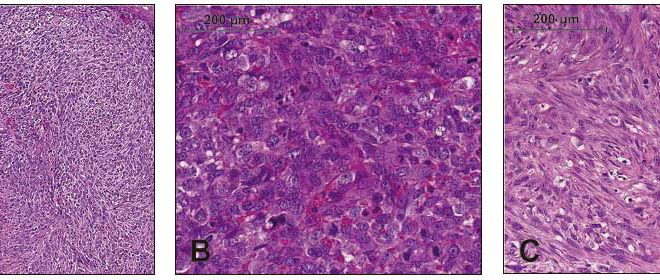
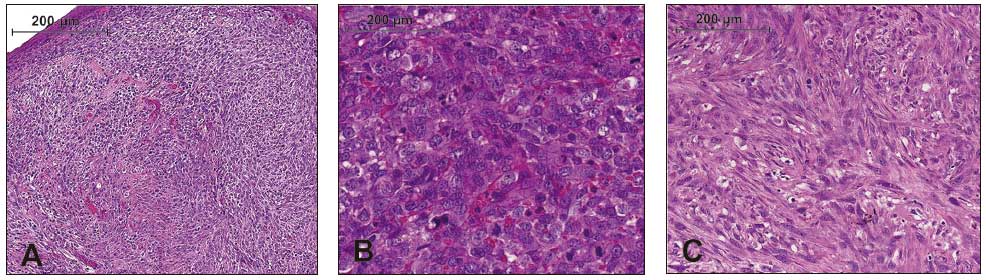
Squamous cell carcinoma was the carcinoma element in all cases. Neoplasms had low grade of cellular differentiation (Table 2). Figure 1 presents microscopy of one of the cases of a mix cancer of squamous cell carcinoma and sarcomatous neoplasm.
Curative intent surgery was performed in 2/6 patients, of which one has been submitted prior to neoadjuvant therapy and is still alive at 13 months of follow-up, with recurrence in vertebral bones.
Most cases were diagnosed in advanced oncologic stages (III and IV), accordingly AJCC 7th Edition.9 Metastasis sites were liver and bones. Nodal spread occurred in 5/6 patients.
Patients 3, 4, 5 and 6 had short survival, and died with disease. Patient who lived longer died at 68 months, without disease.
Table 1. Main characteristics of patients diagnosed with esophageal carcinosarcoma.
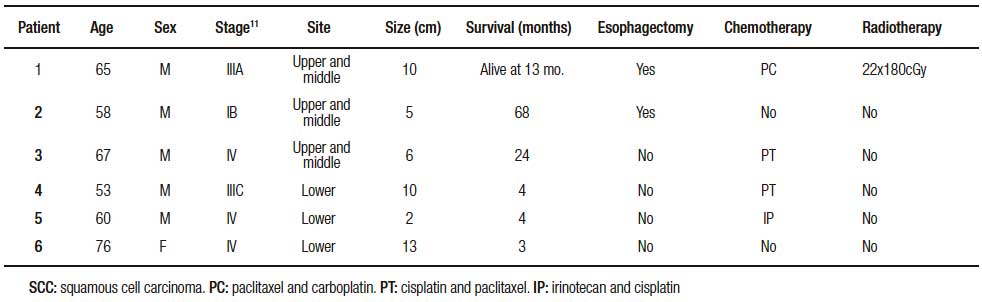
Table 2. Pathology analysis on esophageal carcinosarcoma cases.
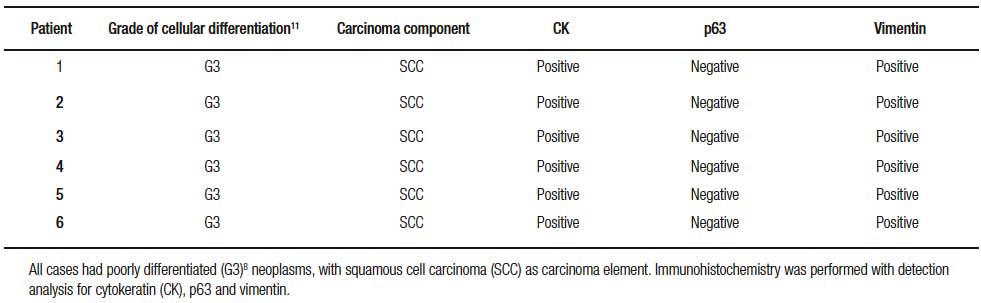
Figure 1. Slides section showing a mixture of epitelioid and sarcomatoid pattern of tumor underlying by a ulcerated epithelium (A, HE, 100x). High power view from the epitelioid (B, HE, 400x) and sarcomatoid component (C, HE, 200x).
Discussion
Esophageal carcinosarcoma is a fairly rare tumor and knowledge about this disease is still scanty. Its origin is unknown. The collision theory claims that epithelial and mesenchymal neoplasms happen to occur at the same time and collide in esophagus. The conversion theory is that high-grade carcinoma cells undergo metaplastic mutation, giving origin to the sarcomatous element. Some theories state that a stem cell would originate epithelial and mesenchymal neoplasms.5, 10-12
Iyomasa et al 5 state that most of the carcinosarcoma tumors are located in the middle or lower esophagus. Macroscopic aspect is usually polypoid. Yamamoto et al 13 affirm that sarcomatoid carcinoma has a much better prognosis than squamous cell carcinoma because these tumors grow into the lumen, with low invasiveness. McCort et al say these tumors usually are diagnosed at early stage, once symptoms tend to be premature.7
Moreover, these tumors would have a low lymph-nodal dissemination incidence.
Our study does not corroborate these statements and suggest a much worse prognosis of this disease. Half of the cases were diagnosed with metastasis. Nodal dissemination was present in most patients. Only one patient survived longer than 2 years of follow-up. Prior to the carcinoma diagnosis, this patient was frequently submitted to endoscopic exams due to Chagasic megaesophagus, leading to an early cancer diagnosis.
Based on previous knowledge on uterus carcinosarcoma, curative resection is the first line treatment option, although there is not enough data in the literature to determine the ideal treatment.14 Supported by the metaplastic carcinoma theory, treatment should be modeled based on treatment protocols for high-risk carcinoma.15
Thereafter, we advocate R0 esophagectomy with strict lymphadenectomy for esophageal carcinosarcoma. Neoadjuvant chemoradiation therapy should be considered. Palliative chemotherapy or radiation therapy could be used in cases of contraindication for surgical resection.
Financial Sustainability. The following study was not sponsored.
References
- Weidner N, Zekan P. Carcinosarcoma of the colon. Report of a unique case with light and immunohistochemical studies. Cancer 1986; 58: 1126-1130.
- Au JT, Sugiyama G, Wang H, Nicastri A, Lee D, Ko W, Tak V. Carcinosarcoma of the oesophagus – a rare mixed type of tumor. JSCR 2010; 7: 1-4.
- Cavallin F, Scarpa M, Alfieri R, Cagol M, Ruol A, Rugge M, Ancona E, Castoro C. Esophageal carcinosarcoma: management and prognosis at a single Italian series. Antic Res 2014; 34: 7455- 7460.
- Hatch GF 3rd, Wertheimer-Hatch L, Hatch KF, Davis GB, Blanchard DK, Foster RS Jr, Skandalakis JE: Tumors of the esophagus. World J Surg 2000; 24: 401-411.
- Iyomasa S, Kato H, Tachimori Y, Watanabe H, Yamaguchi H, Itabashi M: Carcinosarcoma of the esophagus: A twenty-case study. Jpn J Clin Oncol 1990; 20: 99-106.
- Sanada Y, Hihara J, Yoshida K, Yamaguchi Y. Esophageal carcinosarcoma with intramural metastasis. Dis Esophagus 2006; 19: 119-131.
- McCort J. Esophageal carcinosarcoma and pesudosarcoma. Radiology 1972; 102: 519-524.
- Raza MA, Mazzara PF. Sarcomatoid carcinoma of esophagus. Arch Pathol Lab Med 2011; 135: 945-948.
- Rice TW, Blackstone EH, Rusch VW. 7th Edition of AJCC Cancer Staging Manual: Esophagus and Esophagogastric Junction. Ann Surg Oncol 2010; 17: 1721-1724.
- Iwaya T, Maesawa C, Uesugi N, Kimura T, Ogasawara S, Ikeda K, Kimura Y, Mitomo S, Ishida K, Sato N, Saito K, Masuda T. True carcinosarcoma of the esophagus. Dis Esophagus 2006; 19: 48-52.
- Lam KY, Khoo US, Cheung A. Collision of endometrioid carcinoma and stromal sarcoma of the uterus: a report of two cases. Int J Gynecol Pathol 1999; 18: 77-81.
- Singh R. Review literature on uterine carcinosarcoma. J Cancer Res Ther 2014; 10: 461-468.
- Yamamoto Y, Watanabe Y, Horiuchi A, Yoshida M, Yukumi S, Sato K, Nakagawa H, Sugishita H, Ishida N, Furuta S, Kawachi K. True carcinosarcoma of the esophagus: report of a case. Case Rep Gastroenterol 2008; 2: 330-337.
- Callister M, Ramondetta LM, Jhingran A, Burke TW, Eifel PJ. Malignant mixed mullerian tumors of the uterus: analysis of patterns of failure, prognostic factors, and treatment outcome. IJROBP 2004; 58: 786-796.
- Kloos I, Delaloge S, Pautier P, Di Palma M, Goupil A, Duvillard P, Cailleux PE, Lhomme C. Tamoxifen-related uterine carcinosarcomas occur under/after prolonged treatment: report of five cases and review of the literature. Int J Gynecol Cancer 2002; 12: 496-500.
Correspondencia: Francisco Tustumi
Street: Teodoro Sampaio, 632.Code: 05406-000,
Pinheiros, Sao Paulo, Brazil
Phone: +55 11 – 998791048
Email: franciscotustumi@gmail.com
Acta Gastroenterol Latinoam 2017;47(2):122-125
