C V Noejovich1,2 ID· N Bhola3 · J J Blom2,3 ID· M P Temprano4 ID· D Armstrong1,2,3 ID· M I Pinto-Sanchez1,2,3 ID
1McMaster University, Hamilton, ON, L8S 4K1, Canadá.
2Farncombe Family Digestive Health Research Institute, Hamilton, ON, L8S 4K1, Canadá.
3Hamilton Health Sciences, Hamilton, ON, L8S 4K1, Canadá.
4Fundacion Favaloro, Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2026;56(2):135-153
Recibido: 21/05/2026 / Aceptado: 19/06/2026 / Publicado online: 30/06/2026 / https://doi.org/10.52787/agl.v56i2.653

Resumen
La enfermedad celíaca requiere una adherencia estricta a la dieta libre de gluten, lo que puede afectar significativamente las conductas alimentarias y aumentar el riesgo de trastornos de la conducta alimentaria y alimentación desordenada. Si bien resulta clínicamente desafiante, diferenciar estas entidades es fundamental en el contexto de una restricción dietética prescrita. En esta revisión de la literatura, identificamos un mayor riesgo de trastornos de la conducta alimentaria, especialmente de anorexia nerviosa, en personas con enfermedad celíaca, así como conductas de alimentación desordenada, incluyendo restricción excesiva, ansiedad relacionada con los alimentos y evitación social, todas asociadas con una menor calidad de vida. Sin embargo, las herramientas de evaluación actuales no distinguen adecuadamente entre conductas alimentarias patológicas y la adherencia adecuada a una dieta terapéutica prescrita. Aunque se recomienda un abordaje multidisciplinario que incluya apoyo nutricional y de salud mental, aún faltan estrategias terapéuticas específicas basadas en evidencia para la enfermedad. En conjunto, la patología alimentaria en la enfermedad celíaca es frecuente y clínicamente relevante, lo que resalta la necesidad de mejorar su detección y desarrollar herramientas diagnósticas más apropiadas tanto para la práctica clínica como para la investigación.
Palabras claves. Enfermedad celíaca, trastornos de la conducta alimentaria, alimentación desordenada, dieta libre de gluten, anorexia nerviosa, trastorno evitativo/restrictivo de la ingesta alimentaria.
Dietary Restrictions in Celiac Disease: Differential Diagnosis Between Eating Disorders and Disordered Eating
Summary
Celiac disease requires strict adherence to a gluten-free diet, which can significantly affect eating behaviors and increase the risk of eating disorders and disordered eating. Although clinically challenging, distinguishing between these conditions is essential in the context of prescribed dietary restrictions. In this literature review, we identified an increased risk of eating disorders, particularly anorexia nervosa, in individuals with celiac disease, as well as disordered eating behaviors, including excessive restriction, food-related anxiety, and social avoidance, all of which are associated with reduced quality of life. However, current assessment tools do not adequately distinguish between pathological eating behaviors and appropriate adherence to a prescribed therapeutic diet. Although a multidisciplinary approach that includes nutritional and mental health support is recommended, evidence-based therapeutic strategies specific to the condition are still lacking. Overall, eating disorders in celiac disease are common and clinically relevant, highlighting the need to improve their detection and develop more appropriate diagnostic tools for both clinical practice and research.
Keywords. Celiac disease, eating disorders, disordered eating, gluten-free diet, anorexia nervosa, avoidant/restrictive food intake disorder.
Introducción
La enfermedad celíaca (EC) es una enfermedad crónica inmunomediada desencadenada por el gluten -principal complejo proteico presente en el trigo, la cebada y el centeno- que se desarrolla en individuos genéticamente susceptibles.¹ Constituye uno de los trastornos digestivos más frecuentes a nivel mundial y afecta aproximadamente al 1% de la población global.²
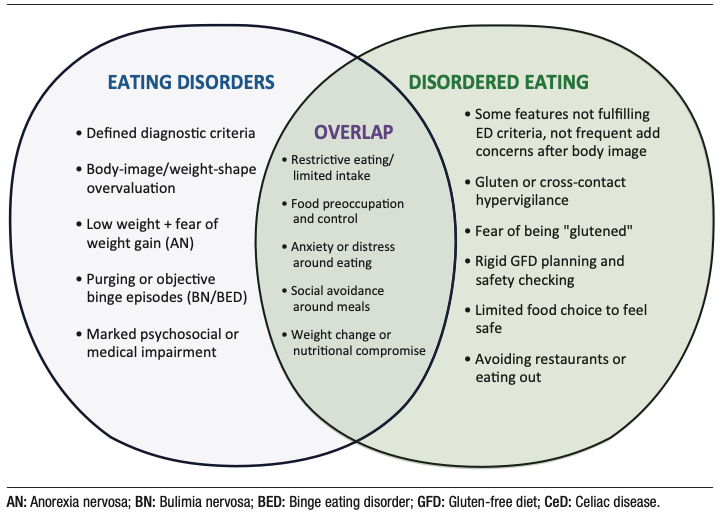
El tratamiento de la EC requiere una adherencia estricta y permanente a una dieta libre de gluten (DLG), ya que incluso exposiciones mínimas al gluten pueden desencadenar una respuesta inmunológica.³ Esta restricción dietética representa una carga sostenida para los pacientes; la relación con los alimentos, las conductas alimentarias y la ansiedad relacionada con la alimentación constituyen factores relevantes para la adherencia terapéutica y la evolución clínica a largo plazo.3 La vigilancia constante necesaria para mantener el cumplimiento de la DLG puede contribuir al desarrollo de alteraciones en la conducta alimentaria, incluyendo la alimentación desordenada (AD).4 Este fenómeno debe diferenciarse de los trastornos de la conducta alimentaria (TCA), entidades psiquiátricas clínicamente definidas que, por lo general, preceden al diagnóstico de EC o se originan a partir de factores psicológicos, sociales o ambientales independientes de esta enfermedad (Figura 1).
Figura 1. Similitudes y diferencias entre los trastornos de la conducta alimentaria y la alimentación desordenada
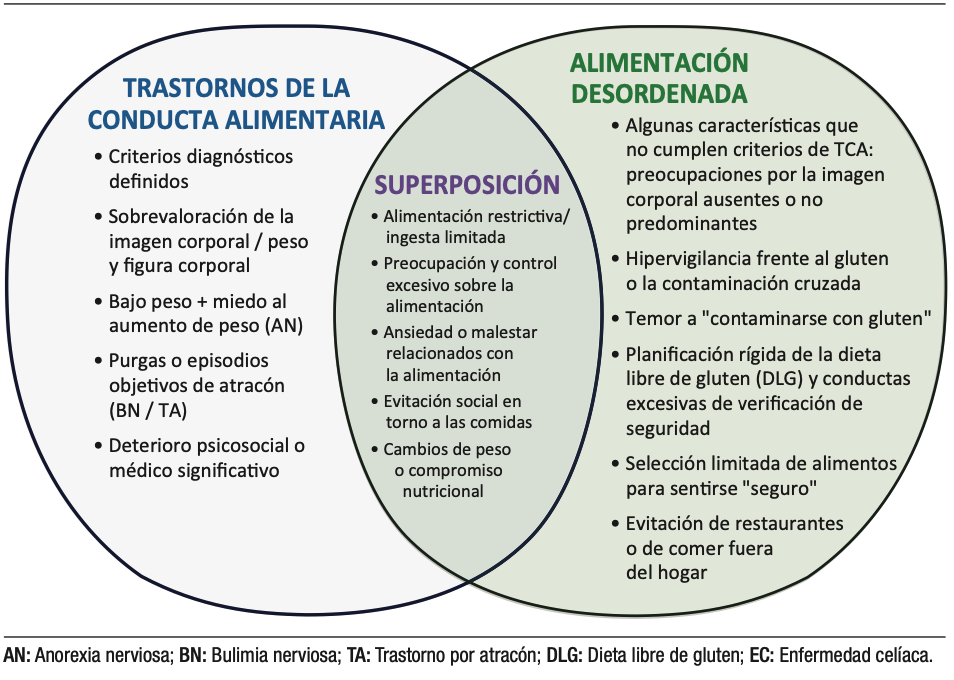
Los TCA son trastornos psiquiátricos caracterizados por alteraciones persistentes de la conducta alimentaria y los pensamientos asociados, con repercusiones médicas significativas y deterioro psicosocial. Las principales categorías diagnósticas incluyen anorexia nerviosa (AN), bulimia nerviosa (BN), trastorno por atracón (TA) y trastorno evitativo/restrictivo de la ingesta alimentaria (ARFID).5 En contraste, la AD comprende un espectro de actitudes y conductas alimentarias desadaptativas, como restricción dietética rígida, ayuno, omisión de comidas o alimentación compulsiva. Aunque estas conductas no cumplen criterios diagnósticos completos para un TCA, pueden asociarse con malestar psicológico, compromiso nutricional y un manejo médico subóptimo.6,7 Esta distinción resulta particularmente relevante en enfermedades gastrointestinales como la EC, la enfermedad inflamatoria intestinal (EII), el síndrome de intestino irritable (SII) y las alergias o intolerancias alimentarias, en las que las restricciones dietéticas médicamente indicadas pueden evolucionar hacia patrones alimentarios excesivamente restrictivos o conductas alimentarias desadaptativas.6,7
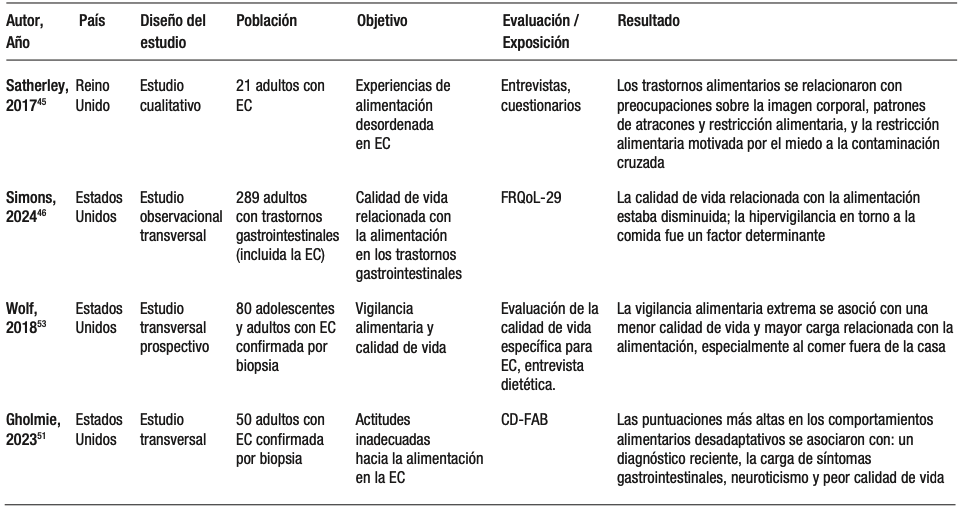
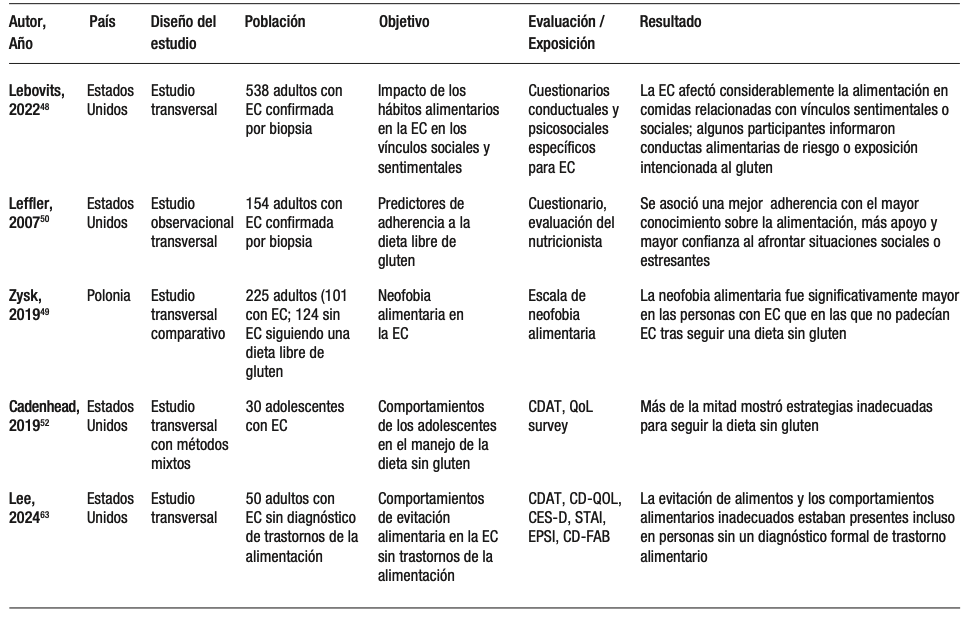
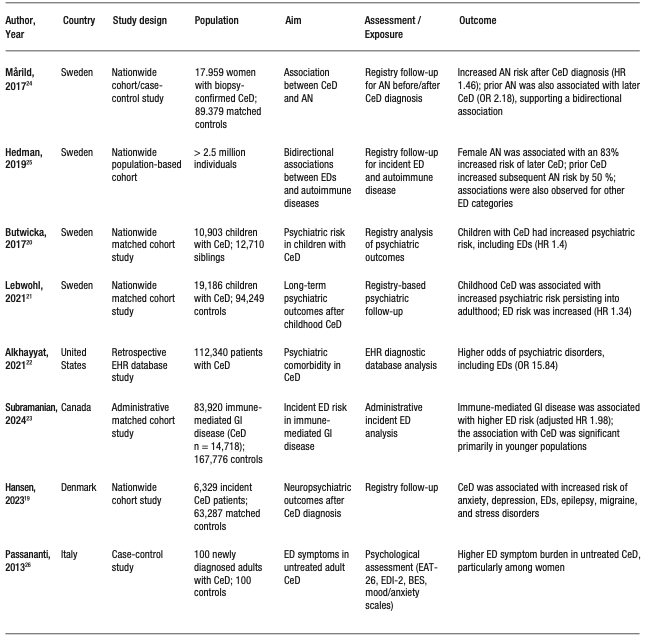
Esta revisión resume la evidencia actual sobre TCA y AD en personas con EC (Tablas 1 y 2), con el objetivo de orientar recomendaciones clínicas e identificar vacíos críticos de conocimiento para futuras investigaciones.
Tabla 1. Estudios sobre trastornos de la conducta alimentaria en la enfermedad celíaca
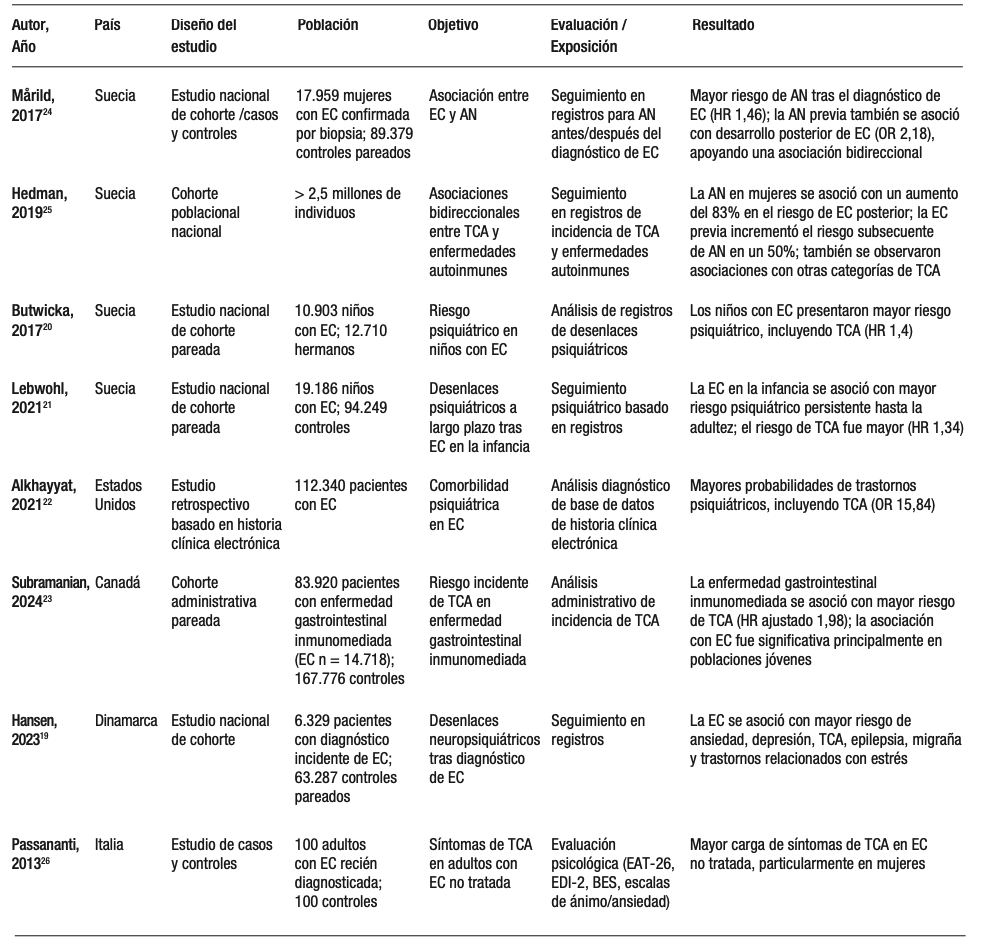
Continuación Tabla 1. Estudios en trastornos de la conducta alimentaria en enfermedad celíaca
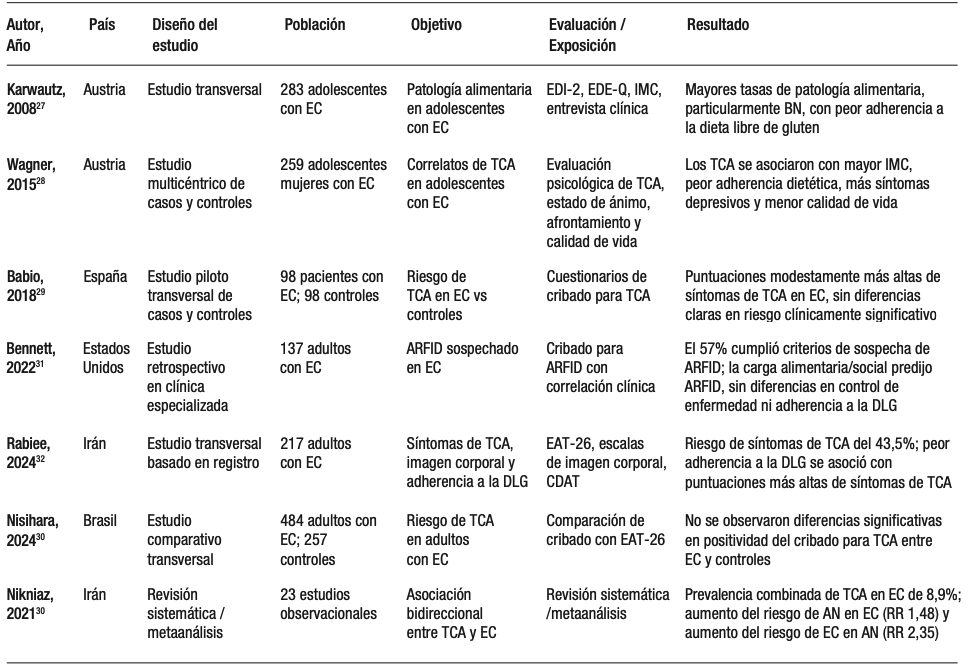
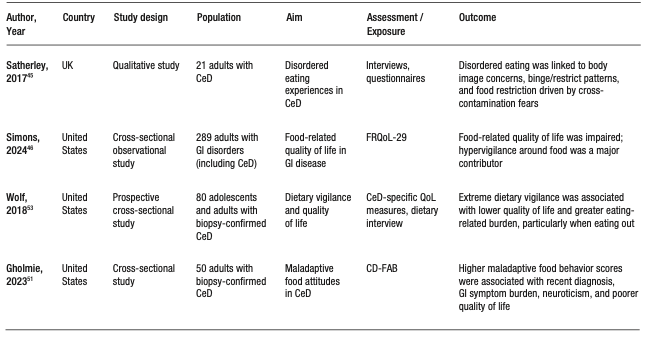
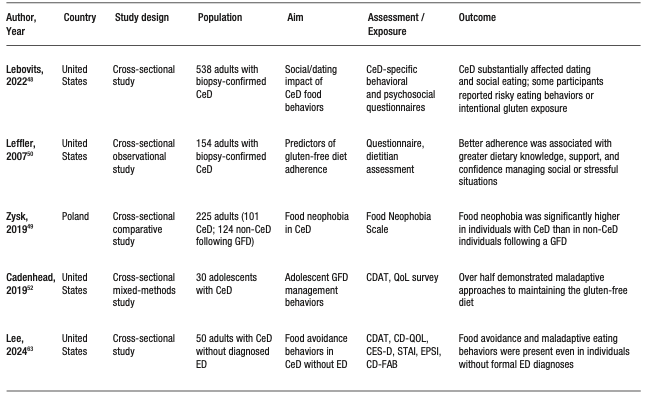
Tabla 2. Estudios sobre alimentación desordenada en la enfermedad celíaca
Continuación Tabla 2. Estudios sobre alimentación desordenada en la enfermedad celíaca
Trastornos de la conducta alimentaria
Los trastornos de la conducta alimentaria (TCA) son trastornos psiquiátricos graves caracterizados por alteraciones persistentes en la conducta alimentaria y en los pensamientos o emociones asociados, que ocasionan deterioro significativo de la salud física y psicosocial.8,9 La prevalencia estimada a lo largo de la vida es de aproximadamente 1 cada 7 hombres y 1 cada 5 mujeres antes de los 40 años; el 95% de los casos incidentes se presentan antes de los 25 años.10
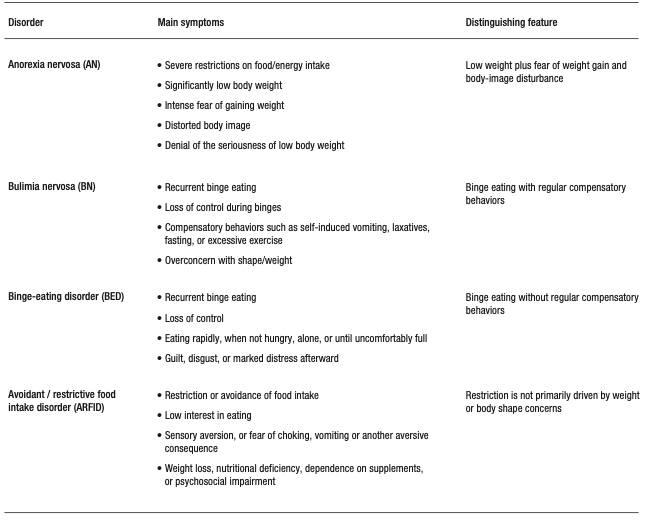
Esta revisión se centra en la anorexia nerviosa (AN), la bulimia nerviosa (BN), el trastorno por atracón (TA) y el trastorno evitativo/restrictivo de la ingesta alimentaria (ARFID), ya que son los diagnósticos más frecuentemente abordados en la investigación y en la práctica clínica relacionadas con la EC (Tabla 3).
La anorexia nerviosa (AN) se caracteriza por una restricción persistente de la ingesta energética que conduce a un peso corporal significativamente bajo, miedo intenso al aumento de peso y alteraciones en la percepción de la imagen corporal, frecuentemente acompañadas de escasa conciencia de la gravedad de la enfermedad y de conductas que interfieren con la recuperación ponderal.8 La AN comprende dos subtipos: el subtipo restrictivo y el subtipo con atracones/purgas, este último caracterizado por episodios recurrentes de atracones y/o conductas purgativas además de una restricción alimentaria severa.8 Las complicaciones son multisistémicas, con frecuente compromiso gastrointestinal.11 Se acompañan de alteraciones cognitivas y emocionales significativas, elevada morbilidad médica y comorbilidad psiquiátrica.8 Estimaciones globales recientes sitúan la prevalencia puntual de AN en aproximadamente 43,9 casos por 100.000 personas (0,04%) en la población general.8 El inicio suele ocurrir en la adolescencia temprana o media, es más frecuente en mujeres y, en general, presenta un pronóstico más favorable en adolescentes que en adultos.12 Cabe destacar que la AN se asocia con una de las tasas de mortalidad más elevadas entre los trastornos psiquiátricos.13
La bulimia nerviosa (BN) se caracteriza por episodios recurrentes de atracones, definidos por la ingesta de una cantidad objetivamente grande de alimentos acompañada de una sensación de pérdida de control, seguidos de conductas compensatorias inapropiadas destinadas a prevenir el aumento de peso, como vómitos autoinducidos, uso indebido de laxantes, ayuno o ejercicio excesivo.8 Para cumplir con los criterios diagnósticos, estas conductas deben presentarse al menos una vez por semana durante un período de tres meses, y la autoevaluación debe estar desproporcionadamente influenciada por el peso y la figura corporal.12 Cuando el individuo presenta un peso significativamente bajo, el diagnóstico se reclasifica como anorexia nerviosa, subtipo con atracones/purgas.13 Estimaciones recientes sitúan la prevalencia global de BN en aproximadamente 156,85 casos por 100.000 personas (0,16%) en la población general.14
Tabla 3. Diagnósticos más frecuentes de trastornos de la conducta alimentaria (TCA) en enfermedad celíaca y síntomas principales75-76
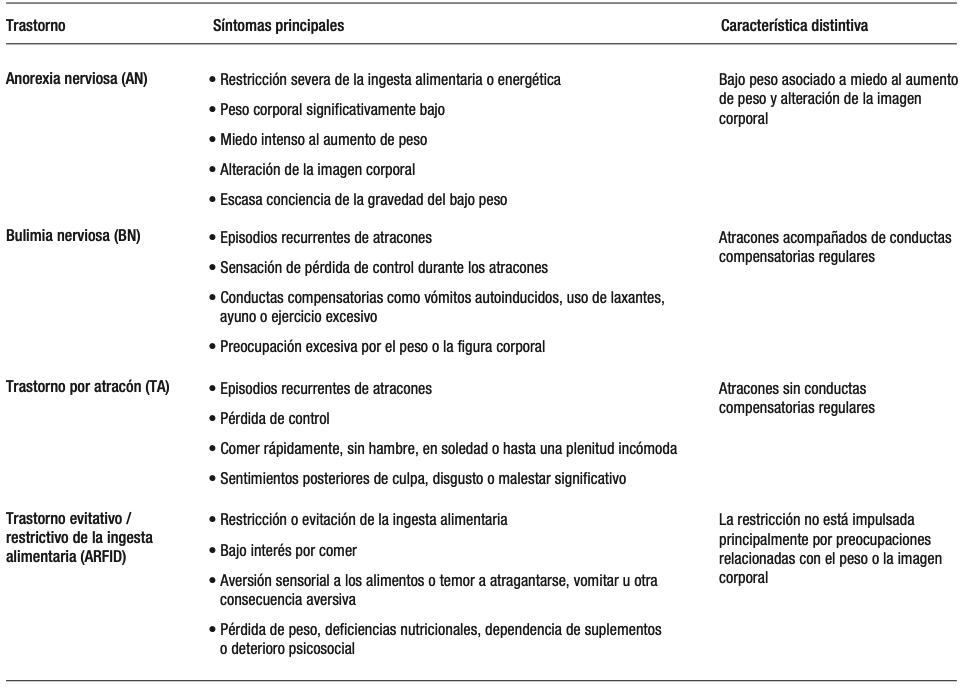
El trastorno por atracón (TA) se caracteriza por episodios recurrentes de atracones en ausencia de conductas compensatorias, con una frecuencia de al menos una vez por semana durante un período mínimo de tres meses.8 Estos episodios suelen incluir el consumo rápido de grandes cantidades de alimentos, ingesta en ausencia de hambre fisiológica, alimentación hasta alcanzar una sensación de plenitud incómoda y malestar emocional significativo, incluyendo sentimientos de vergüenza, culpa o ánimo depresivo.13 El TA es aproximadamente dos veces más frecuente en mujeres que en hombres y representa el trastorno de la conducta alimentaria más prevalente. Su prevalencia global estimada es de 1,9%, alcanzando 2,6% en estudios realizados en Estados Unidos, y representa aproximadamente el 47% de todos los diagnósticos de trastornos de la conducta alimentaria.15,16
El trastorno evitativo/restrictivo de la ingesta alimentaria (ARFID) es un trastorno de la conducta alimentaria caracterizado por evitación o restricción persistente de la ingesta alimentaria que conduce a una incapacidad para satisfacer los requerimientos nutricionales. Tiene consecuencias clínicamente significativas, que incluyen pérdida de peso, deficiencias nutricionales, dependencia de suplementos o terapias de soporte nutricional, y deterioro psicosocial, en ausencia de preocupación por el peso corporal o la imagen corporal.8 El ARFID puede manifestarse como alimentación altamente selectiva, bajo apetito, evitación alimentaria basada en características sensoriales o restricción impulsada por ansiedad o temor ante consecuencias aversivas, como atragantamiento o vómitos.13 El ARFID difiere de la alimentación desordenada (AD), un término que describe conductas o actitudes alimentarias problemáticas, como la evitación alimentaria o la restricción dietética, que pueden ser transitorias o dependientes del contexto y que no necesariamente ocasionan deterioro nutricional, funcional o psicosocial clínicamente significativo.
Datos poblacionales de Estados Unidos indican que las personas con trastornos de la conducta alimentaria definidos según los criterios del DSM-5, incluidos AN, BN, TA y ARFID, presentan tasas más altas de comorbilidad psiquiátrica concurrente, en particular trastornos del estado de ánimo, trastornos de ansiedad, trastornos por consumo de sustancias y trastornos de la personalidad. Entre estas comorbilidades, el trastorno depresivo mayor es el más frecuente, seguido por el trastorno por consumo de alcohol.17
La Tabla 3 resume los trastornos de la conducta alimentaria más frecuentes en la enfermedad celíaca.
Trastornos de la conducta alimentaria en la enfermedad celíaca
La asociación entre los trastornos de la conducta alimentaria (TCA) y la enfermedad celíaca (EC) muestra variabilidad entre los estudios disponibles. Un metaanálisis y revisión sistemática18 reportaron una prevalencia combinada de TCA del 8,88% en personas con EC e identificaron una relación bidireccional entre ambas condiciones, siendo la asociación más fuerte y consistente la observada con la anorexia nerviosa (AN). Estudios poblacionales, tanto en cohortes adultas19 como pediátricas,20 también han demostrado un mayor riesgo de TCA en personas con EC. De manera similar, Lebwohl et al.21 describieron un mayor riesgo de TCA tanto antes como después del diagnóstico de EC, lo que respalda una relación temporal compleja y bidireccional. Asimismo, grandes estudios basados en bases de datos administrativas de Estados Unidos y Ontario sugieren que las personas con EC presentan un riesgo leve a sustancialmente aumentado de diagnóstico de TCA en comparación con controles, con incrementos reportados de aproximadamente 1,5 a 2 veces, dependiendo de la población estudiada y del subtipo de TCA.22,23
Los estudios de cohortes poblacionales aportan evidencia más específica sobre la asociación bidireccional entre EC y AN. Un estudio nacional sueco mostró que las personas con EC confirmada por biopsia presentaban un riesgo aproximadamente 1,4 a 1,5 veces mayor de desarrollar AN en comparación con la población general. A la inversa, las personas con diagnóstico previo de AN presentaban un riesgo aproximadamente 2 veces mayor de desarrollar EC posteriormente.24 Estos hallazgos fueron replicados por Hedman et al.,25 lo que refuerza la consistencia del vínculo epidemiológico entre EC y AN.
La presentación clínica de los TCA en la EC es altamente heterogénea. En adultos con EC no tratada, se han reportado puntuaciones más elevadas en síntomas relacionados con trastornos alimentarios, particularmente en mujeres, con puntuaciones en el Eating Attitudes Test (EAT-26) aproximadamente 1,5 a 2 veces superiores a las observadas en controles.26 En adolescentes, se han descripto mayores tasas de bulimia nerviosa (BN) y un espectro más amplio de patología alimentaria (entre 10 y 15% en algunas cohortes), con EC precediendo al inicio del TCA en la mayoría de los casos.27 En adolescentes con EC, la presencia de TCA comórbidos se asoció con un mayor índice de masa corporal (IMC), más síntomas depresivos y una peor calidad de vida en comparación con aquellos sin TCA.28 La asociación con un IMC más elevado sugiere que la alteración alimentaria en esta población no se limita exclusivamente a fenotipos restrictivos con bajo peso.
No obstante, los hallazgos de los estudios de casos y controles han sido inconsistentes. Por ejemplo, Babio et al.29 reportaron únicamente diferencias leves en las puntuaciones de cribado para TCA entre personas con EC y controles, mientras que Nisihara et al.30 no encontraron diferencias significativas en el riesgo de TCA. Más recientemente, el ARFID ha emergido como un fenotipo clínicamente relevante en EC, con un estudio que reportó que más de la mitad de los adultos con EC cumplían criterios de sospecha de ARFID,31 impulsados principalmente por la ansiedad relacionada con los alimentos y la carga social asociada a la alimentación.
La relación entre la alimentación desordenada (AD) y la adherencia a la dieta libre de gluten también parece compleja. Aunque podría esperarse que fenotipos restrictivos como la AN o el ARFID se asocien con una mayor rigidez dietética y con una mayor adherencia a la DLG, Rabiee et al.32 encontraron que puntuaciones más elevadas de síntomas compatibles con TCA se asociaban de manera significativa con una menor adherencia a la DLG.
En conjunto, estos hallazgos sugieren una mayor carga de síntomas de TCA en subgrupos de personas con EC, aunque las estimaciones varían considerablemente según el diseño del estudio, la población evaluada y los métodos de medición empleados. La evidencia más consistente respalda una relación bidireccional entre EC y AN, mientras que las asociaciones con otros subtipos de TCA siguen siendo menos robustas.
Diagnóstico y evaluación de los trastornos de la conducta alimentaria en la enfermedad celíaca
El diagnóstico es fundamentalmente clínico y debe basarse en los criterios del DSM-5-TR, más que en los instrumentos de cribado.8 Aunque los TCA pueden presentarse en personas de cualquier edad, género u origen étnico, los adolescentes y adultos jóvenes constituyen los grupos de mayor riesgo, y la AN suele manifestarse a edades más tempranas que la BN.33
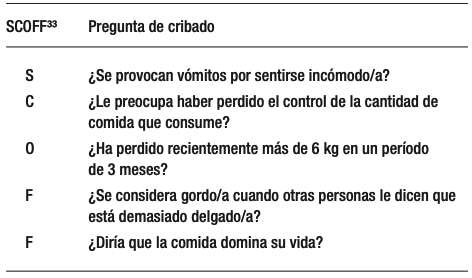
Una evaluación integral debe incluir el análisis de los cambios ponderales a lo largo del tiempo, los patrones de restricción alimentaria o atracones, el uso de conductas compensatorias (Tabla 3) y las actitudes asociadas con la alimentación y la imagen corporal, junto con el cribado de comorbilidades psiquiátricas y médicas.8,9 La evaluación también debe considerar la motivación del paciente para el tratamiento y la disponibilidad de apoyo psicosocial.12 Herramientas breves de cribado, como el SCOFF (Tabla 4),34 pueden ser útiles como primer paso; sin embargo, un resultado positivo requiere una evaluación diagnóstica confirmatoria por un profesional de salud mental, idealmente un psiquiatra.13,35 La confirmación diagnóstica puede apoyarse en entrevistas estructuradas como el Eating Disorder Examination (EDE)36 y el Eating Disorder Assessment for DSM-5 (EDA-5).37 Asimismo, instrumentos autoadministrados como el Eating Disorder Inventory (EDI-3)38 pueden ser útiles para el seguimiento de síntomas y la evaluación longitudinal.39 Dado el potencial de inestabilidad médica asociado a los TCA, que incluyen bradicardia, hipotensión, alteraciones electrolíticas, deshidratación o signos de malnutrición, el riesgo médico debe evaluarse de manera sistemática ante la sospecha de un TCA, con derivación a niveles de atención de mayor complejidad cuando esté clínicamente indicado.13,40
Tabla 4. Cuestionario SCOFF34 para cribado de trastornos de la conducta alimentaria en la práctica clínica
Manejo clínico de los trastornos de la conducta alimentaria en enfermedad celíaca
El manejo de los TCA en personas con EC requiere un enfoque dual, que integre el tratamiento médico estricto de la EC con intervenciones terapéuticas basadas en la evidencia para los TCA. Esta superposición plantea desafíos clínicos relevantes, ya que la adherencia a la DLG puede, de forma inadvertida, reforzar patrones de alimentación restrictivos u obsesivos. En consecuencia, la atención debe brindarse mediante un equipo multidisciplinario integrado, con el objetivo de garantizar mensajes consistentes, minimizar temores innecesarios relacionados con los alimentos y diferenciar claramente entre las restricciones dietéticas médicamente indicadas y las conductas restrictivas patológicas impulsadas por el TCA. Al igual que en pacientes sin EC, el manejo eficaz de los TCA en personas con EC se basa en un enfoque multidisciplinario coordinado, con un tratamiento individualizado según el diagnóstico específico, la edad, el estado nutricional y el riesgo médico del paciente. La colaboración entre médicos, nutricionistas y profesionales de la salud mental es esencial, y el diagnóstico precoz, junto con una intervención oportuna basada en la evidencia, se asocia con mejores desenlaces clínicos.9,13,40 En la AN, los objetivos terapéuticos principales incluyen la rehabilitación nutricional y la restauración ponderal, combinadas con psicoterapia específica para el trastorno; en adolescentes y adultos jóvenes con apoyo familiar o de cuidadores, el tratamiento basado en la familia constituye la estrategia de elección.9,12,40 La terapia cognitivo-conductual (TCC) constituye el tratamiento de primera línea para BN, y puede considerarse la fluoxetina como tratamiento coadyuvante o alternativa terapéutica eficaz cuando esté clínicamente indicada.35,40 En el TA, la terapia conductual (TC) y la psicoterapia interpersonal han demostrado una eficacia sólida, tanto en formato individual como grupal, y pueden considerarse los antidepresivos en casos seleccionados.41,42 El manejo del ARFID se centra en restaurar una ingesta nutricional adecuada, corregir deficiencias nutricionales, ampliar la variedad dietética y abordar las conductas de evitación mediante intervenciones conductuales, terapias basadas en exposición, terapia cognitivo-conductual y tratamiento basado en la familia.41,42 La evidencia para el tratamiento del ARFID sigue siendo más limitada que para otros TCA, y actualmente no existe un enfoque terapéutico universalmente consensuado. En términos generales, se recomienda un modelo de atención escalonado y coordinado, en el que la intensidad del tratamiento se ajuste al nivel de riesgo clínico, integrando de manera simultánea apoyo médico, nutricional y psicológico.35,40,42,43
Alimentación desordenada en la enfermedad celíaca
En la EC, la adherencia estricta a la DLG plantea desafíos particulares que pueden influir de manera significativa en las conductas alimentarias.4,44-46 La necesidad de vigilancia constante, incluyendo la revisión minuciosa del etiquetado, la prevención de contaminación cruzada y la gestión de situaciones sociales relacionadas con la alimentación pueden favorecer una mayor monitorización de la ingesta y ansiedad relacionadas con los alimentos.4,47 Aunque estas conductas son adaptativas y médicamente necesarias, en algunos individuos evolucionan hacia patrones desadaptativos que se asemejan a la AD, tales como restricción excesiva, rigidez conductual o evitación de comer fuera del hogar.46,48-51 La evidencia emergente sugiere una interacción compleja entre la EC y las conductas de AD, con posibles implicancias sobre el bienestar psicológico y la calidad de vida. Se ha demostrado que las personas con EC presentan tasas más elevadas de neofobia alimentaria en comparación con individuos sin EC, definida como temor o evitación de alimentos nuevos o desconocidos, y de ortorexia nerviosa (ON), caracterizada por una preocupación patológica por consumir alimentos percibidos como saludables, puros o “limpios”. En esas situaciones se encuentran conductas dietéticas restrictivas, evitación alimentaria, malestar emocional cuando dichas conductas se transgreden y potencial deterioro nutricional o psicosocial.49 En la EC, la distinción entre AN y ON puede ser desafiante, dado que la evitación médicamente apropiada del gluten puede asemejarse a conductas ortoréxicas; la preocupación clínica surge cuando la restricción alimentaria se vuelve excesiva, impulsada por ansiedad, nutricionalmente perjudicial o se extiende más allá de lo médicamente necesario. Satherley et al.45 reportaron puntuaciones elevadas de síntomas compatibles con AD en poblaciones con EC, incluyendo tanto conductas restrictivas como episodios de alimentación compulsiva. De manera similar, Cadenhead et al.,52 encontraron que más de la mitad de los adolescentes con EC presentaban patrones alimentarios desadaptativos, como rigidez, preocupación excesiva por los alimentos y evitación alimentaria, los cuales se asociaron con disminución de la calidad de vida.
La vigilancia dietética en sí misma parece contribuir a la carga de enfermedad. La vigilancia adaptativa en el mantenimiento de una DLG implica conductas proporcionales y flexibles que favorecen un manejo seguro de la enfermedad, mientras que la hipervigilancia se caracteriza por una monitorización excesiva impulsada por ansiedad, que conduce a restricciones innecesarias, deterioro social o disminución de la calidad de vida. Estudios en distintas enfermedades gastrointestinales, incluida la EC, han demostrado que el control dietético estricto se asocia con mayor hipervigilancia relacionada con la alimentación y con un impacto negativo en la calidad de vida relacionada con los alimentos.46-48 En cohortes específicas de EC,51-53 una mayor adherencia a la DLG se ha asociado con una mayor percepción de carga y menor calidad de vida, mientras que actitudes alimentarias desadaptativas evaluadas mediante herramientas como la escala Celiac Disease Food Attitudes and Behaviors (CD-FAB) se correlacionan con desenlaces menos favorables reportados por los pacientes.
Las implicancias sociales de la adherencia a la DLG agravan aún más esta carga. Lebovits et al.48 reportaron que el 68,4% de las personas con EC percibían un impacto moderado a elevado del diagnóstico en su vida afectiva, incluyendo dudas respecto a la intimidad física e incomodidad al discutir necesidades dietéticas en contextos públicos, lo que contribuyó a episodios de no adherencia intencional. De forma similar, Leffler et al.50 encontraron que la adherencia a la DLG afectaba negativamente el funcionamiento social, con un 44,2% de los participantes que evitaban comer fuera del hogar y un 21,4% que evitaban participar en eventos sociales. Estos factores pueden contribuir tanto a la no adherencia intencional como al desarrollo o al mantenimiento de conductas alimentarias desadaptativas.
En conjunto, la evidencia actual sugiere que, aunque la vigilancia dietética es esencial para el manejo de la EC, también puede predisponer a un subgrupo de individuos al desarrollo de conductas de AD, con implicancias relevantes para el bienestar psicológico y la calidad de vida. La Tabla 3 resume los estudios sobre las conductas de alimentación desordenada en la enfermedad celíaca.
Diagnóstico y evaluación de la alimentación desordenada en la enfermedad celíaca
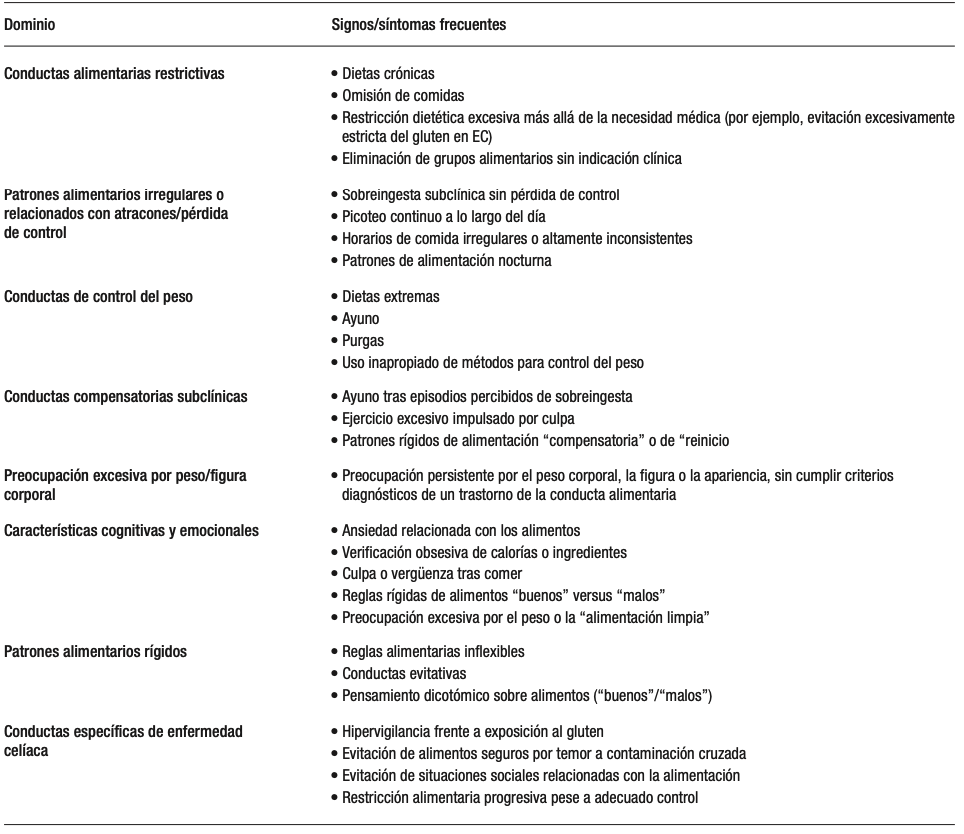
La evaluación de la AD en la EC requiere una cuidadosa diferenciación entre la adherencia adaptativa a la DLG y las conductas alimentarias restrictivas desadaptativas que exceden la necesidad médica. Dado que la AD es un concepto que engloba actitudes o conductas alimentarias problemáticas que pueden ser subclínicas o dependientes del contexto, la evaluación debe incluir el análisis de la rigidez dietética, el temor a la exposición al gluten, la ansiedad relacionada con los alimentos, el deterioro psicosocial, el estado nutricional y el impacto de estas conductas en el funcionamiento cotidiano. Ejemplos de conductas de AD se presentan en la Tabla 5. Herramientas como la escala Celiac Disease Food Attitudes and Behaviors (CD-FAB) pueden ser útiles para identificar cogniciones y conductas alimentarias desadaptativas relacionadas con los alimentos; sin embargo, no permiten establecer un diagnóstico psiquiátrico formal. Es fundamental considerar y descartar, cuando corresponda, la presencia de un TCA incluyendo AN, BN, TA o ARFID, dado que estas entidades constituyen diagnósticos psiquiátricos definidos que requieren abordajes terapéuticos específicos.
Tabla 5. Ejemplos de conductas de alimentación desordenada77-78
Manejo de alimentación desordenada en enfermedad celíaca
Actualmente no existen marcos terapéuticos específicos para la EC dirigidos al manejo de la AD. La literatura disponible respalda un enfoque multidisciplinario orientado a la prevención, que integre atención médica, nutricional y psicológica, junto con educación continua y monitoreo longitudinal.52,54,55 En contextos donde no se dispone de atención multidisciplinaria integral, un modelo pragmático mínimo de atención debería incluir un médico tratante (gastroenterólogo o médico de atención primaria) responsable de la evaluación clínica y el monitoreo médico, un nutricionista con experiencia en EC que oriente un manejo seguro y nutricionalmente adecuado de la DLG, y derivación a un profesional de salud mental, cuando esté disponible, ante la sospecha de factores psicológicos subyacentes o de un TCA, con escalamiento a atención especializada según la gravedad clínica y el riesgo médico.49-50 Dado que el pilar del tratamiento de la EC es la adherencia estricta y de por vida a la DLG, los clínicos deben equilibrar cuidadosamente la necesidad de evitar estrictamente el gluten con el riesgo de reforzar patrones alimentarios desadaptativos o favorecer la progresión hacia un TCA formal.56,57 En la EC, la AD puede surgir como consecuencia de restricción alimentaria impulsada por síntomas, hipervigilancia definida como monitorización, preocupación o conductas de evitación excesivas o desproporcionadas frente al riesgo de ingestión accidental de gluten o contaminación cruzada, más allá de lo razonablemente necesario para un manejo seguro de la enfermedad, o temor a consecuencias adversas,56,57 todos fenómenos amplificados por las exigencias de una adherencia dietética estricta.44,58 En este contexto, el seguimiento clínico debe incluir evaluaciones estructuradas y repetidas de los patrones alimentarios y su contexto, evitando asumir automáticamente que una restricción progresiva refleja adherencia adecuada o, en el extremo opuesto, etiquetarla prematuramente como patología psiquiátrica.47,56
La evaluación clínica debe extenderse más allá de la adherencia a la DLG e incluir patrones sugestivos de alimentación desadaptativa, tales como omisión de comidas, ayuno para evitar síntomas, reducción progresiva de la variedad dietética, evitación de alimentos seguros, temor a comer fuera del hogar, dependencia excesiva de alimentos preparados exclusivamente por el propio paciente y preocupación persistente por los alimentos. Otros hallazgos de preocupación incluyen pérdida de peso no intencional, alteraciones de la imagen corporal, conductas compensatorias (por ejemplo, purgas o uso de laxantes) y persistencia de síntomas gastrointestinales a pesar de una restricción dietética progresivamente más estricta.56,58
Existe información muy limitada sobre la implementación rutinaria de herramientas formales de cribado para TCA o AD en clínicas de EC, y actualmente no existe ninguna guía clínica que recomiende el cribado universal y estandarizado de TCA/AD en todos los pacientes con EC. Sin embargo, algunos instrumentos pueden ser útiles para la identificación de casos en individuos de mayor riesgo, incluyendo herramientas generales para TCA como el Eating Disorder Screen for Primary Care (ESP)59 y el cuestionario SCOFF,34 así como también instrumentos específicos para EC, como la escala Celiac Disease Food Attitudes and Behaviors (CD-FAB),60 que puede contribuir a identificar actitudes y conductas alimentarias desadaptativas relacionadas con los alimentos.
El manejo nutricional debe ser realizado por nutricionistas con experiencia tanto en EC como en TCA, con el objetivo de mantener una exclusión estricta del gluten y minimizar las restricciones innecesarias. Esto incluye promover la variedad dietética dentro de la DLG, clarificar la diferencia entre restricciones médicamente indicadas y conductas evitativas, y abordar temores relacionados con la alimentación, como la contaminación cruzada. Las intervenciones psicológicas constituyen un componente central del tratamiento y deben orientarse a modificar cogniciones y conductas desadaptativas relacionadas con los alimentos, la seguridad alimentaria y la imagen corporal. En este contexto, pueden adaptarse estrategias basadas en evidencia, como la terapia cognitivo-conductual (TCC) y el tratamiento basado en la familia, para abordar características superpuestas con entidades como el ARFID y AN.
Las consideraciones del desarrollo también son relevantes, ya que las conductas alimentarias desadaptativas suelen surgir durante la adolescencia.61 En personas con EC, factores de riesgo tempranos como la insatisfacción con el peso corporal, los síntomas de ansiedad o depresión y las dinámicas familiares en torno a las comidas pueden interactuar con las exigencias crónicas de la DLG, perpetuando o exacerbando conductas de AD hasta la adultez.45,62 Cuando se identifican conductas de AD, los clínicos deben evaluar la estabilidad médica e iniciar la derivación precoz a profesionales de la salud mental, idealmente con experiencia en TCA y familiaridad con las enfermedades gastrointestinales.56 Finalmente, es esencial mantener mensajes consistentes y coordinados entre las distintas disciplinas para evitar reforzar patrones alimentarios impulsados por el miedo o restricciones excesivas.
Desafíos nutricionales en el manejo de los trastornos de la conducta alimentaria y la alimentación desordenada en la enfermedad celíaca
El manejo de los TCA, particularmente AN, BN y ARFID en personas con dietas restrictivas médicamente prescritas, como ocurre en la EC, plantea una paradoja terapéutica singular. El tratamiento estándar de los TCA busca reducir las reglas dietéticas rígidas, desafiar la evitación alimentaria y restaurar la flexibilidad en la relación con la alimentación, mientras que la EC exige adherencia estricta y permanente a una dieta libre de gluten (DLG), lo que genera una tensión inherente entre la recuperación psicológica y la necesidad médica.26,63 Esta dificultad es particularmente relevante en fenotipos restrictivos de TCA, en los que la DLG puede reforzar inadvertidamente cogniciones restrictivas o incluso integrarse al trastorno como una forma socialmente aceptable de evitación.64,65
Desde una perspectiva nutricional, mantener una DLG estricta mientras se trabaja para normalizar los patrones alimentarios resulta intrínsecamente complejo. La DLG requiere la exclusión completa del trigo, centeno, cebada y cereales relacionados, además de la vigilancia constante de fuentes ocultas de gluten y de la contaminación cruzada durante el procesamiento, almacenamiento y preparación de alimentos. Sin una orientación adecuada, esta vigilancia necesaria puede derivar en una restricción alimentaria excesiva. Por ello, el manejo nutricional debe enfatizar sustituciones nutricionalmente adecuadas, libres de gluten, que incluyan cereales integrales, así como una planificación alimentaria equilibrada que garantice una ingesta suficiente de energía y nutrientes.
Esto es particularmente importante dada la limitada calidad nutricional de muchos productos comerciales libres de gluten, que con frecuencia no están fortificados con micronutrientes como hierro, folato, tiamina, riboflavina y niacina. En un estudio de Jamieson et al.,66 los productos básicos libres de gluten contenían 1,3 veces más grasa, así como niveles significativamente menores de hierro (-55%), folato (-44%) y proteínas (-36%) en comparación con sus equivalentes con gluten. La variabilidad en el contenido y la composición de la fibra, particularmente la fermentable, también puede contribuir a la persistencia de síntomas gastrointestinales y afectar negativamente el bienestar psicológico en personas con EC.67
La vulnerabilidad nutricional puede verse aún más agravada en pacientes con TCA coexistente, en los que la ingesta insuficiente, la eliminación de grupos alimentarios, las conductas de atracón-purga y los patrones alimentarios erráticos pueden exacerbar deficiencias de micronutrientes comúnmente observadas en ambas condiciones, como hierro, vitaminas del complejo B y ácidos grasos esenciales.65,68 Las alteraciones en los patrones alimentarios también pueden contribuir a disbiosis del microbioma intestinal, empeorando potencialmente los síntomas gastrointestinales y dificultando la adherencia dietética.69 En fenotipos no restrictivos, (como la BN y el TA), los episodios de ingesta descontrolada pueden aumentar el riesgo de exposición inadvertida al gluten, particularmente cuando las opciones libres de gluten son limitadas.64,68
La AD en la EC presenta desafíos nutricionales superpuestos pero distintos. A diferencia de los TCA, la AD en EC suele estar impulsada por ansiedad relacionada con los síntomas, temor a la exposición al gluten o vigilancia dietética excesiva, más que por preocupaciones relacionadas con la imagen corporal. Los pacientes pueden eliminar progresivamente alimentos más allá de lo médicamente necesario, reduciendo la diversidad dietética y aumentando el riesgo de afectación nutricional a pesar de mantener adherencia a la DLG.65,66 La hipervigilancia frente a la contaminación cruzada y la dependencia de una variedad limitada de alimentos percibidos como “seguros” pueden deteriorar aún más la calidad de vida y reforzar conductas evitativas.63,65,70 El acceso a un nutricionista especializado en EC puede ayudar a reducir el riesgo de superposición de restricciones dietéticas, fenómeno en el que los pacientes adoptan progresivamente múltiples restricciones alimentarias innecesarias además de la DLG, incrementando la ansiedad relacionada con la alimentación, el compromiso nutricional y la carga psicosocial.71
Los cambios de peso tras el inicio de la DLG pueden complicar aún más el manejo clínico. La recuperación ponderal en individuos previamente desnutridos, o el aumento de peso asociado a una mejor absorción intestinal y mayor disponibilidad de productos ultraprocesados libres de gluten, puede contribuir a preocupaciones relacionadas con la imagen corporal, desencadenando conductas de AD o exacerbando TCA preexistentes, especialmente en adolescentes y adultos jóvenes.63,70 Es necesario utilizar herramientas educativas estandarizadas y basadas en evidencia, incluyendo listas de verificación para contaminación cruzada.72,73
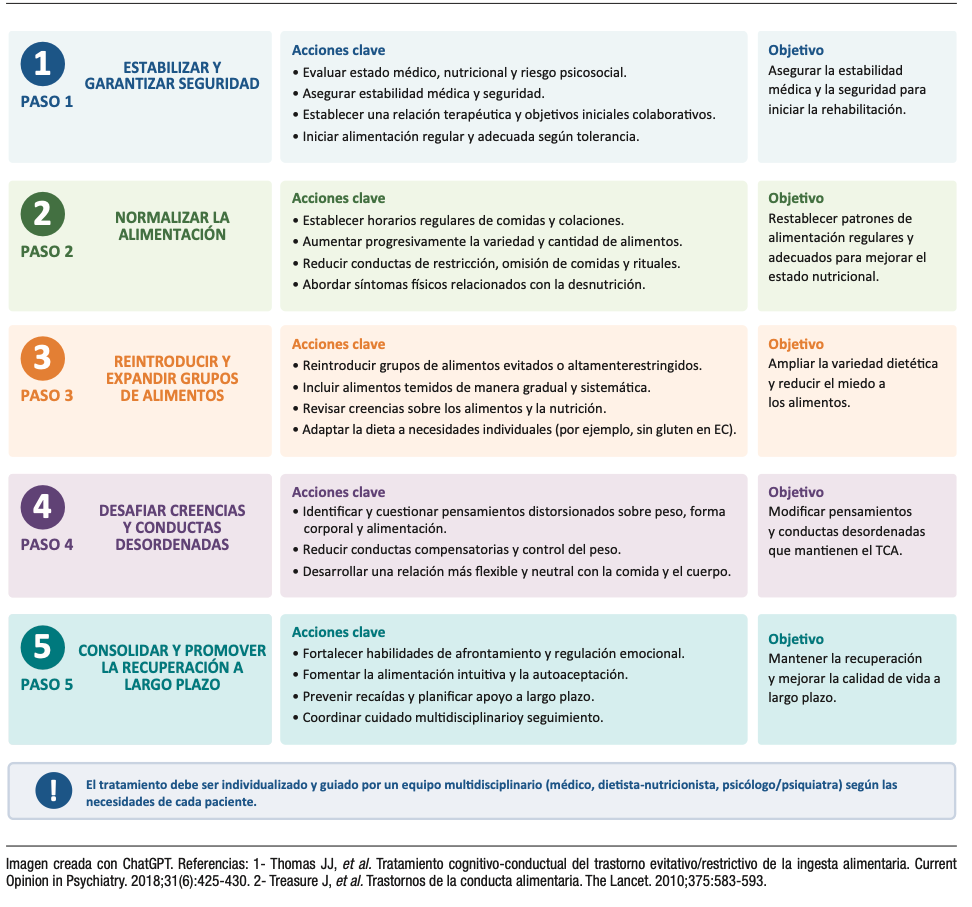
Desde una perspectiva práctica, una jerarquía de objetivos nutricionales para el manejo de la AD comienza con la adecuación nutricional, priorizando la restauración de una ingesta energética consistente y suficiente, dado que la alimentación insuficiente o errática puede agravar los síntomas gastrointestinales, aumentar la ansiedad relacionada con los alimentos y reforzar conductas restrictivas. Una vez alcanzada una ingesta adecuada, el foco debe orientarse hacia el equilibrio nutricional, asegurando comidas con un aporte suficiente de carbohidratos, proteínas y grasas para favorecer la saciedad, la adecuación nutricional y una función digestiva más predecible. El siguiente paso es la variedad dietética, que promueve la expansión gradual más allá de una variedad limitada de alimentos considerados “seguros”, con el fin de mejorar la diversidad alimentaria, la calidad nutricional y la confianza al comer. Solo una vez consolidadas estas bases, debería abordarse la reintroducción de alimentos específicos temidos o evitados, mediante un enfoque gradual y estructurado de rehabilitación alimentaria (Figura 2). Este modelo escalonado se adapta a los principios establecidos de la rehabilitación nutricional en TCA, priorizando la restauración de una ingesta adecuada, una nutrición equilibrada, la variedad dietética y la reintroducción progresiva de alimentos temidos.
Figura 2. Recomendaciones escalonadas para la rehabilitación nutricional en pacientes con conductas alimentarias desordenadas
Recomendaciones para el manejo clínico de los trastornos de la conducta alimentaria y de la alimentación desordenada en la enfermedad celíaca
Esta sección proporciona una orientación práctica para los clínicos involucrados en el manejo de los TCA y los AD en personas con EC, con énfasis en la toma de decisiones clínicas y la delimitación de roles dentro del equipo asistencial.
En pacientes con restricción alimentaria, ansiedad relacionada con los alimentos, cambios de peso o malestar asociado a la DLG, la primera tarea clínica consiste en determinar si estas manifestaciones corresponden a una AD o a un TCA que requiera evaluación especializada en salud mental. Distinguir entre una adherencia adaptativa a la DLG y patrones de AD o de un TCA formal puede ser complejo, ya que la restricción médicamente necesaria puede superponerse a conductas desadaptativas o patológicas. Herramientas breves, como el cuestionario SCOFF,34 o el Cuestionario de Examen de Trastornos de la Conducta Alimentaria (EDE-Q)74 pueden facilitar la identificación temprana en el ámbito clínico. La presencia de restricción alimentaria severa con bajo peso, miedo al aumento de peso, atracones, conductas compensatorias o alteración significativa de la imagen corporal sugiere un TCA formal, mientras que la hipervigilancia, las conductas rígidas orientadas a la “seguridad alimentaria” o la reducción progresiva de las opciones alimentarias pueden reflejar AD.
Cuando se sospecha un TCA, el rol del médico consiste en reconocer los signos de alarma, evaluar la estabilidad médica y facilitar una derivación oportuna a salud mental o a programas especializados en TCA. Los TCA requieren un manejo psiquiátrico especializado, mientras que las intervenciones centradas exclusivamente en la nutrición pueden resultar insuficientes o incluso reforzar inadvertidamente conductas desadaptativas. Por ambos motivos es fundamental la derivación temprana.
En pacientes con AD que no cumplen los criterios diagnósticos de TCA, el médico y el nutricionista asumen un rol más activo en el manejo. El tratamiento debe centrarse en mantener una exclusión estricta del gluten minimizando restricciones innecesarias, garantizar la adecuación nutricional y abordar creencias desadaptativas relacionadas con los alimentos. Cuando los pacientes muestran resistencia a involucrarse en servicios de salud mental, los clínicos deben mantener un seguimiento longitudinal, documentar las preocupaciones clínicas y reconsiderar la derivación utilizando un lenguaje claro, no estigmatizante y centrado en la funcionalidad, la seguridad y la calidad de vida.
Dentro de este marco, varias recomendaciones prácticas pueden orientar el manejo clínico:
1. Evaluar la gravedad y el contexto de las alteraciones alimentarias para diferenciar la AD de un TCA formal.
2. Indicar derivación temprana cuando existan características compatibles con TCA, malestar psicológico significativo o riesgo nutricional.
3. Favorecer la colaboración multidisciplinaria con nutricionistas y profesionales de la salud mental
con experiencia tanto en EC como en TCA.
4. Reforzar la educación basada en evidencia sobre la DLG para prevenir restricciones excesivas o innecesarias.
5. Reconocer la carga psicológica de la vigilancia dietética crónica, particularmente en contextos sociales y situaciones de incertidumbre alimentaria.
6. Monitorear longitudinalmente las conductas alimentarias, el estado nutricional y el impacto psicosocial.
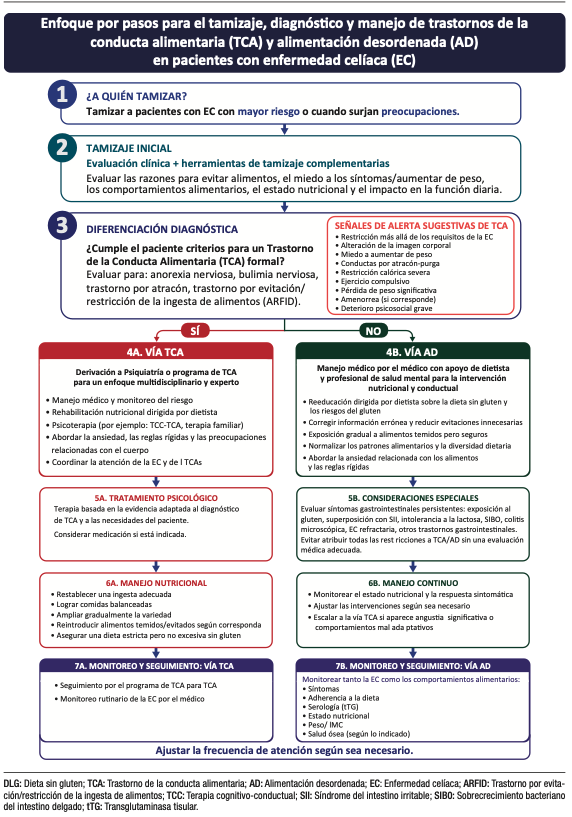
En conjunto, el manejo debe ser individualizado y multidisciplinario, con una delimitación clara de roles entre las especialidades. En la Figura 3 se presenta un resumen del diagnóstico y manejo de los TCA y la AD en la enfermedad celíaca.
Abordaje de la hipervigilancia en la enfermedad celíaca
La hipervigilancia ante la exposición al gluten merece una atención particular en el manejo de la enfermedad celíaca. Si bien los pacientes deben desarrollar habilidades prácticas para mantener una dieta libre de gluten, que incluyen la lectura de etiquetas, la prevención de la contaminación cruzada y la selección segura de alimentos, en algunos individuos estas conductas pueden volverse excesivamente rígidas o impulsadas por el miedo. En estos casos, la educación del paciente constituye un componente central del manejo. El asesoramiento claro y basado en evidencia por parte del equipo clínico o de un nutricionista especializado en enfermedad celíaca puede ayudar a corregir conceptos erróneos sobre el riesgo real de exposición al gluten, diferenciar escenarios de alto y bajo riesgo y reducir la incertidumbre relacionada con el etiquetado alimentario, la contaminación cruzada y las prácticas seguras al comer fuera del hogar.
El uso de herramientas educativas estandarizadas, listas de verificación prácticas y mensajes consistentes entre los distintos profesionales de la salud puede contribuir a disminuir temores innecesarios y evitar recomendaciones contradictorias que refuercen la ansiedad.30-32
Las estrategias conductuales también pueden ser útiles, particularmente cuando la hipervigilancia conduce a una restricción progresiva o al deterioro psicosocial. La reintroducción gradual de alimentos seguros innecesariamente evitados, la expansión de la variedad dietética y la exposición acompañada a situaciones sociales de alimentación de bajo riesgo pueden ayudar a reconstruir la confianza y reducir la dependencia de un repertorio limitado de alimentos percibidos como “seguros”. El objetivo no es disminuir la adherencia a la DLG, sino promover una vigilancia proporcionada, entendida como el mantenimiento de la seguridad médica, minimizando al mismo tiempo las restricciones innecesarias, la ansiedad relacionada con los alimentos y el deterioro de la calidad de vida.
La Figura 3 resume un enfoque escalonado para el cribado, diagnóstico y manejo de los trastornos de la conducta alimentaria y la alimentación desordenada en la enfermedad celíaca.
Figura 3. Enfoque escalonado para el tamizaje, diagnóstico y manejo de los trastornos de la conducta alimentaria y la alimentación desordenada en la enfermedad celíaca
Discusion
La intersección entre la enfermedad celíaca, las conductas alimentarias desadaptativas o alimentación desordenada y los trastornos de la conducta alimentaria representa un desafío clínico relevante e insuficientemente reconocido en gastroenterología. Estas condiciones pueden simularse, enmascararse o exacerbarse mutuamente, dado que comparten manifestaciones clínicas superpuestas, como cambios de peso, dolor abdominal, alteraciones del tránsito intestinal, fatiga, deficiencias de micronutrientes y malnutrición.8 En consecuencia, distinguir entre actividad intestinal persistente, falta de adherencia dietética y coexistencia de AD o TCA puede resultar particularmente difícil, especialmente en aquellos pacientes con síntomas persistentes o compromiso nutricional a pesar de una adherencia estricta a la DLG.
Esta complejidad se ve amplificada por el hecho de que el tratamiento de la EC es intrínsecamente dietético. Aunque la adherencia estricta a la DLG es esencial, la vigilancia constante requerida puede contribuir al desarrollo de hipervigilancia, rigidez conductual y ansiedad relacionada con los alimentos en individuos susceptibles, con un potencial de evolución hacia patrones alimentarios desadaptativos. A la inversa, los TCA preexistentes pueden interferir con la adherencia terapéutica, la rehabilitación nutricional y la interpretación clínica de los síntomas. Estas dinámicas evidencian la importancia de diferenciar el manejo dietético adaptativo de la restricción patológica como componente central del cuidado de la EC. En este contexto, los TCA y la AD deben reconocerse como factores clínicamente relevantes que influyen en la adherencia, la persistencia de síntomas, el riesgo nutricional y la calidad de vida, lo que justifica un abordaje multidisciplinario que involucre a gastroenterólogos, nutricionistas y profesionales de salud mental.
Los factores psicosociales parecen desempeñar un papel central en esta interacción. Una mayor carga de síntomas compatibles con TCA se ha asociado con síntomas depresivos, menor calidad de vida, mayor carga social e insatisfacción corporal.28,30–32 Estos hallazgos respaldan un modelo biopsicosocial; sin embargo, la direccionalidad de estas asociaciones sigue sin estar claramente definida, dado que el malestar psicosocial podría actuar como factor contribuyente o ser consecuencia de conductas alimentarias desadaptativas. Se requieren estudios prospectivos longitudinales que permitan esclarecer las relaciones temporales, identificar predictores de progresión desde AD hacia TCA formales y determinar si las intervenciones psicosociales dirigidas pueden mejorar los desenlaces clínicos y la calidad de vida en personas con EC.
Persisten importantes faltas de evidencia científica. En primer lugar, existe escasa orientación sobre cómo adaptar las intervenciones nutricionales en pacientes con coexistencia de EC y AD o TCA. El asesoramiento dietético convencional, cuando se brinda de forma aislada, puede resultar insuficiente o incluso reforzar inadvertidamente conductas restrictivas o impulsadas por el miedo. En segundo lugar, falta evidencia centrada en el tratamiento. La mayoría de los estudios disponibles son transversales u observacionales y no evalúan la eficacia de modelos de atención integrados. Aún no está claro si los tratamientos estándar para TCA requieren modificaciones en el contexto de la EC, ni cuál es la mejor estrategia para coordinar la atención gastroenterológica, nutricional y psiquiátrica.
En tercer lugar, existe una carencia de herramientas validadas específicamente diseñadas para distinguir las conductas alimentarias desadaptativas de las restricciones dietéticas médicamente necesarias. Los instrumentos existentes (por ejemplo, EAT-26, SCOFF) fueron desarrollados para poblaciones generales y pueden tener especificidad limitada en condiciones que requieren modificaciones dietéticas terapéuticas, como la EC, las alergias alimentarias, la enfermedad inflamatoria intestinal, los trastornos gastrointestinales eosinofílicos o el síndrome de intestino irritable manejado con dietas de eliminación. Aunque herramientas específicas como la escala Celiac Disease Food Attitudes and Behaviors (CD-FAB), muestran potencial para identificar cogniciones y conductas alimentarias desadaptativas en EC, se requiere mayor validación y una implementación clínica más amplia.51,60
Finalmente, el papel de los determinantes sociales de la salud (DSS), incluyendo el acceso a alimentos, la alfabetización en salud y el apoyo social, permanece escasamente explorado, a pesar de su probable influencia en la vulnerabilidad a desarrollar AD en personas con EC.
Las investigaciones futuras deberían priorizar estudios longitudinales que aclaren las relaciones temporales entre EC, AD y TCA, así como ensayos de intervención que evalúen modelos de atención multidisciplinarios e integrados. El desarrollo de herramientas de evaluación específicas para EC y la incorporación de marcos conceptuales basados en los determinantes sociales de la salud serán fundamentales para optimizar tanto la atención clínica como la investigación en esta población.
Propiedad intelectual. Los autores declaran que los datos, las figuras y tablas presentes en el manuscrito son originales y se realizaron en sus instituciones pertenecientes.
Financiamiento. David Armstrong cuenta con el apoyo de la Cátedra Douglas de Investigación en Nutrición. MIPS cuenta con el apoyo de la Iniciativa de Nutrición del Farncombe Family Digestive Health Research Institute.
Conflictos de interes. María Inés Pinto-Sanchez ha recibido financiamiento para investigación de Celiac Canada, Takeda y Provention Bio, así como una subvención educativa de Takeda. MIPS es miembro del Scientific Medical. Advisory Board de Celiac Canada.
Aviso de derechos de autor

© 2026 Acta Gastroenterológica Latinoamericana. Este es un artículo de acceso abierto publicado bajo los términos de la Licencia Creative Commons Attribution (CC BY-NC-SA 4.0), la cual permite el uso, la distribución y la reproducción de forma no comercial, siempre que se cite al autor y la fuente original.
Cite este artículo como: Noejovich C V, Bholan N, Blom J J y col. Restricción alimentaria en la enfermedad celíaca: diagnóstico diferencial entre trastornos de la conducta alimentaria y alimentación desordenada. Acta Gastroenterol Latinoam. 2026;56(2):135-153. https://doi.org/10.52787/agl.v56i2.653
Referencias
- Catassi C, Verdu EF, Bai JC, Lionetti E. Coeliac disease. Lancet. 2022;399(10344):2413-2426. DOI:10.1016/S0140-6736(22) 00794-2
- Singh P, Arora A, Strand TA, et al. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16(6):823-36.e2. DOI:10.1016/j.cgh.2017.06.037
- Hallert C, Grännö C, Hultén S, et al. Living with coeliac disease: controlled study of the burden of illness. Scand J Gastroenterol. 2002;37(1):39-42. DOI:10.1080/003655202753387338
- de Rosa A, Troncone A, Vacca M, Ciacci C. Characteristics and quality of illness behavior in celiac disease. Psychosomatics. 2004;45(4):336-342. DOI:10.1176/appi.psy.45.4.336
- American Psychiatric Association. What are eating disorders? Psychiatry.org. Accessed March 17, 2026. https://www.psychiatry.org/patients-families/eating-disorders/what-are-eating-disorders
- Peters JE, Basnayake C, Hebbard GS, Salzberg MR, Kamm MA. Prevalence of disordered eating in adults with gastrointestinal disorders: A systematic review. Neurogastroenterology and Motil. 2022;34(8):e14278. DOI:10.1111/nmo.14278
- Staller K, Abber SR, Burton Murray H. The intersection between eating disorders and gastrointestinal disorders: a narrative review and practical guide. Lancet Gastroenterol Hepatol. 2023;8(6):565-578. DOI:10.1016/S2468-1253(22)00351-X
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, text rev (DSM-5-TR). Washington, DC: American Psychiatric Association Publishing; 2022.
- Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. 2020;395(10227):899-911. DOI:10.1016/S0140-6736(20)30059-3
- Ward ZJ, Bleich SN, Cradock AL, et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. JAMA Netw Open. 2019;2(10):e1912925. DOI:10.1001/jamanetworkopen.2019.12925
- Schalla MA, Stengel A. Gastrointestinal alterations in anorexia nervosa – A systematic review. Eur Eat Disord Rev. 2019;27(5):447-461. DOI:10.1002/erv.2679
- Zipfel S, Giel KE, Bulik CM, Hay P, Schmidt U. Anorexia nervosa: aetiology, assessment, and treatment. Lancet Psychiatry. 2015;2(12):1099-1111. DOI:10.1016/S2215-0366(15)00356-9
- Academy for Eating Disorders (AED) Medical Care Standards Committee. Eating Disorders: A Guide to Medical Care. 4th ed. Reston, VA: Academy for Eating Disorders;2021.
- Shen Y, Chen B, Zhang H, Shen W, Wu C, Jiang L. Global, regional, and national burden of eating disorders in 204 countries and territories, 1990-2021: findings from the Global Burden of Disease Study 2021. J Eat Disord. 2025;13(1):290. Published 2025 Dec 20. DOI:10.1186/s40337-025-01492-8
- Mars JA, Iqbal A, Rehman A. Binge Eating Disorder. In: StatPearls. StatPearls Publishing; 2026. Updated August 11, 2024. Accessed May 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK551700/
- Santomauro DF, Melen S, Mitchison D, Vos T, Whiteford H, Ferrari AJ. The hidden burden of eating disorders: an extension of estimates from the Global Burden of Disease Study 2019. Lancet Psychiatry. 2021;8(4):320-328. DOI:10.1016/S2215-0366
(21)00040-7 - Udo T, Grilo CM. Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States.Int J Eat Disord. 2019;52(1):42-50. DOI:10.1002/eat.23004
- Nikniaz Z, Beheshti S, Abbasalizad Farhangi M, Nikniaz L. A systematic review and meta-analysis of the prevalence and odds of eating disorders in patients with celiac disease and vice-versa. Int J Eat Disord. 2021;54(9):1563-1574. DOI:10.1002/eat.23561
- Hansen S, Osler M, Thysen SM, Rumessen JJ, Linneberg A, Kårhus LL. Celiac disease and risk of neuropsychiatric disorders: A nationwide cohort study. Acta Psychiatr Scand. 2023;148(1):60-70. DOI:10.1111/acps.13554
- Butwicka A, Lichtenstein P, Frisén L, Almqvist C, Larsson H, Ludvigsson JF. Celiac Disease Is Associated with Childhood Psychiatric Disorders: A Population-Based Study. J Pediatr. 2017;
184:87-93.e1. DOI:10.1016/j.jpeds.2017.01.043 - Lebwohl B, Haggård L, Emilsson L, et al. Psychiatric Disorders in Patients with a Diagnosis of Celiac Disease During Childhood From 1973 to 2016. Clin Gastroenterol Hepatol. 2021;19(10):2093-2101.e13. DOI:10.1016/j.cgh.2020.08.018
- Alkhayyat M, Qapaja T, Aggarwal M, et al. Epidemiology and risk of psychiatric disorders among patients with celiac disease: A population-based national study. J Gastroenterol Hepatol. 2021;36(8):2165-2170. DOI:10.1111/jgh.15437
- Subramanian L, Coo H, Jane A, et al. Celiac Disease and Inflammatory Bowel Disease Are Associated with Increased Risk of Eating Disorders: An Ontario Health Administrative Database Study. Clin Transl Gastroenterol. 2024;15(5):e00700. Published 2024 May 1. DOI:10.14309/ctg.0000000000000700
- Mårild K, Størdal K, Bulik CM, et al. Celiac Disease and Anorexia Nervosa: A Nationwide Study. Pediatrics. 2017;139(5):
e20164367. DOI:10.1542/peds.2016-4367 - Hedman A, Breithaupt L, Hübel C, et al. Bidirectional relationship between eating disorders and autoimmune diseases. J Child Psychol Psychiatry. 2019;60(7):803-812. DOI:10.1111/jcpp.12958
- Passananti V, Siniscalchi M, Zingone F, et al. Prevalence of eating disorders in adults with celiac disease. Gastroenterol Res Pract. 2013;2013:491657. DOI:10.1155/2013/491657
- Karwautz A, Wagner G, Berger G, Sinnreich U, Grylli V, Huber WD. Eating pathology in adolescents with celiac disease. Psychosomatics. 2008;49(5):399-406. DOI:10.1176/appi.psy.49.5.399
- Wagner G, Zeiler M, Berger G, et al. Eating Disorders in Adolescents with Celiac Disease: Influence of Personality Characteristics and Coping. Eur Eat Disord Rev. 2015;23(5):361-370. DOI:10.1002/erv.2376
- Babio N, Alcázar M, Castillejo G, et al. Risk of Eating Disorders in Patients With Celiac Disease. J Pediatr Gastroenterol Nutr. 2018;66(1):53-57. DOI:10.1097/MPG.0000000000001648
- Nisihara R, Techy ACM, Staichok C, et al. Prevalence of eating disorders in patients with celiac disease: a comparative study with healthy individuals. Rev Assoc Med Bras (1992). 2024;70(1):e20231090. Published 2024 Mar 15. DOI:10.1590/
1806-9282.20231090 - Bennett A, Bery A, Esposito P, Zickgraf H, Adams DW. Avoidant/Restrictive Food Intake Disorder Characteristics and Prevalence in Adult Celiac Disease Patients. Gastro Hep Adv. 2022;1(3):321-327. Published 2022 Mar 30. DOI:10.1016/j.gastha.2022.01.002
- Rabiee R, Mahdavi R, Shirmohammadi M, Nikniaz Z. Eating disorders, body image dissatisfaction and their association with gluten-free diet adherence among patients with celiac disease. BMC Nutr. 2024;10(1):100. Published 2024 Jul 18. DOI:10.1186/s40795-024-00910-5
- Litmanen J, Fröjd S, Marttunen M, Isomaa R, Kaltiala-Heino R. Are eating disorders and their symptoms increasing in prevalence among adolescent population? Nord J Psychiatry. 2017;71(1):61-66. DOI:10.1080/08039488.2016.1224272
- Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. 1999;319(7223):1467-1468. DOI:10.1136/bmj.319.7223.1467
- National Institute for Health and Care Excellence. Eating disorders: recognition and treatment (NG69). NICE. Published May 23, 2017. Exceptional surveillance updated 2024. Accessed March 17, 2026. https://www.nice.org.uk/guidance/ng69
- Fairburn CG, Cooper Z, O’Connor ME. Eating Disorder Examination. Edition 17.0D. CBT-E website. Published January 2014. Accessed May 14, 2026. https://www.cbte.co/for-professionals/measures/
- Sysko R, Glasofer DR, Hildebrandt T, et al. The eating disorder assessment for DSM-5 (EDA-5): development and validation of a structured interview for feeding and eating disorders. Int J Eat Disord. 2015;48(5):452-463. DOI:10.1002/eat.22388
- Garner DM. Eating Disorder Inventory-3: Professional Manual. Psychological Assessment Resources; 2004.
- Schaefer LM, Crosby RD, Machado PPP. A systematic review of instruments for the assessment of eating disorders among adults. Curr Opin Psychiatry. 2021;34(6):543-562. DOI:10.1097/YCO.0000000000000746
- Crone C, Fochtmann LJ, Attia E, et al. The American Psychiatric Association practice guideline for the treatment of patients with eating disorders. Am J Psychiatry. 2023;180(2):167-171. DOI:10.1176/appi.ajp.23180001
- Kambanis PE, Thomas JJ. Assessment and Treatment of Avoidant/Restrictive Food Intake Disorder. Current Psychiatry Reports. 2023;25(2):53-64. DOI:10.1007/s11920-022-01404-6
- Ramirez Z, Gunturu S. Avoidant Restrictive Food Intake Disorder. In: StatPearls. StatPearls Publishing; 2024. Updated May 1, 2024.
- Di Cara M, Rizzo C, Corallo F, et al. Avoidant Restrictive Food Intake Disorder: A Narrative Review of Types and Characteristics of Therapeutic Interventions.Children (Basel). 2023;10(8):1297. Published 2023 Jul 28. DOI:10.3390/children10081297
- Coburn S, Germone M, McGarva J, Taft T. Psychological Considerations for Food Intolerances: Celiac Sprue, Eosinophilic Esophagitis, and Non-Celiac Gluten Sensitivity. Gastroenterol Clin North Am. 2022;51(4):753-764. DOI:10.1016/j.gtc.2022.07.003
- Satherley RM, Higgs S, Howard R. Disordered eating patterns in coeliac disease: a framework analysis. J Hum Nutr Diet. 2017;30(6):724-736. DOI:10.1111/jhn.12475
- Simons M, McGarva J, Doerfler B, et al. Food-related quality of life driven by hypervigilance and anxiety around eating in organic gastrointestinal conditions. J Hum Nutr Diet. 2024;37(6):1505-1515. DOI:10.1111/jhn.13358
- Lee AR, Zybert P, Chen Z, et al. Food avoidance beyond the gluten-free diet and the association with quality of life and eating attitudes and behaviors in adults with celiac disease. Nutrients. 2024;16(19):3411. DOI:10.3390/nu16193411
- Lebovits J, Lee AR, Ciaccio EJ, et al. Impact of Celiac Disease on Dating. Dig Dis Sci. 2022;67(11):5158-5167. DOI:10.1007/s10620-022-07548-y
- Zysk W, Glabska D, Guzek D. Food Neophobia in Celiac Disease and Other Gluten-Free Diet Individuals. Nutrients. 2019;11(8):1762. Published 2019 Jul 31. DOI:10.3390/nu11081762
- Leffler DA, Dennis M, Edwards George JB, Kelly CP. The interaction between eating disorders and celiac disease: an exploration of 10 cases. Eur J Gastroenterol Hepatol. 2007;19(3):251-255. DOI:10.1097/MEG.0b013e328012db37
- Gholmie Y, Lee AR, Satherley RM, et al. Maladaptive Food
Attitudes and Behaviors in Individuals with Celiac Disease and Their Association with Quality of Life. Dig Dis Sci. 2023;68(7):2899-2907. DOI:10.1007/s10620-023-07912-6 - Cadenhead JW, Lee AR, Nguyen TTT, Lebwohl B, Green PHR, Wolf RL. Dietary Adherence to Recommendations among a Cohort of Adults and Teens with Celiac Disease Maintaining a Gluten-Free Diet Compared to a Nationally Representative Sample: A Cross-Sectional Study. Nutrients. 2024;16(18):3067. Published 2024 Sep 11. DOI:10.3390/nu16183067
- Wolf RL, Lebwohl B, Lee AR, et al. Hypervigilance to a Gluten-Free Diet and Decreased Quality of Life in Teenagers and Adults with Celiac Disease. Dig Dis Sci. 2018;63(6):1438-1448. DOI:10.1007/s10620-018-4936-4
- Rajani S, Sawyer-Bennett J, Shirton L, et al. Patient and parent
satisfaction with a dietitian- and nurse- led celiac disease clinic for children at the Stollery Children’s Hospital, Edmonton, Alberta. Can J Gastroenterol. 2013;27(8):463-466. DOI:10.1155/2013/537160 - Mulder CJJ, Elli L, Lebwohl B, et al. Follow-Up of Celiac Disease in Adults: «When, What, Who, and Where». Nutrients. 2023;15(9):2048. Published 2023 Apr 24. DOI:10.3390/nu15092048
- Riehl ME, Scarlata K. Understanding disordered eating risks in patients with gastrointestinal conditions. J Acad Nutr Diet. 2022;122(3):491-499. DOI:10.1016/j.jand.2021.03.001
- Ciao AC, Loth K, Neumark-Sztainer D. Preventing eating disorder pathology: common and unique features of successful eating disorders prevention programs. Curr Psychiatry Rep. 2014;16(7):453. DOI:10.1007/s11920-014-0453-0
- Quick VM, Byrd-Bredbenner C, Neumark-Sztainer D. Chronic illness and disordered eating: a discussion of the literature. Adv Nutr. 2013;4(3):277-286. DOI:10.3945/an.112.003608
- Cotton MA, Ball C, Robinson P. Four simple questions can help screen for eating disorders. J Gen Intern Med. 2003;18(1):53-56. DOI:10.1046/j.1525-1497.2003.20374.x
- Satherley RM, Howard R, Higgs S. Development and validation of the Coeliac Disease Food Attitudes and Behaviours Scale. Gastroenterol Res Pract. 2018;2018:6930269. DOI:10.1155/2018/6930269
- Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27:281-295. DOI:10.1038/s41380-021-01161-7
- Rowen K, Solomon P, Tebbett-Mock A. Psychosocial predictors of disordered eating in adolescents with celiac disease: a cross-sectional study. Child Health Care. Published online 2026.
DOI:10.1080/02739615.2026.2626386 - Lee AR, Lebwohl B, Lebovits J, Wolf RL, Ciaccio EJ, Green PHR. Factors associated with maladaptive eating behaviors, social anxiety, and quality of life in adults with celiac disease. Nutrients. 2021;13(12):4494. DOI:10.3390/nu13124494
- Wei Y, Wang Y, Yuan Y, Chen J. Celiac disease, gluten-free diet, and eating disorders: from bench to bedside. Foods. 2025;14(1):74. DOI:10.3390/foods14010074
- Bennett A, Bery A, Esposito P, Zickgraf H, Adams DW. Avoidant/restrictive food intake disorder characteristics and prevalence in adult celiac disease patients. Gastro Hep Adv. 2022;1(3):
321-327. DOI:10.1016/j.gastha.2022.01.002 - Jamieson JA, Weir M, Gougeon L. Canadian packaged gluten-free foods are less nutritious than their regular gluten-containing counterparts. PeerJ. 2018;6:e5875. DOI:10.7717/peerj.5875
- Roncoroni L, Bascuñán KA, Doneda L, et al. A low FODMAP gluten-free diet improves functional gastrointestinal disorders and overall mental health of celiac disease patients: a randomized controlled trial. Nutrients. 2018;10(8):1023. DOI:10.3390/nu10081023
- Kaul R, Jansson-Knodell C, Simons ML, Weekley K, Gardinier D, Rubio-Tapia A. Avoidant/restrictive food intake disorder in celiac disease. Nutrients. 2025;17:3197. DOI:10.3390/nu17203197
- Kleiman SC, Watson HJ, Bulik-Sullivan EC, et al. The intestinal microbiota in anorexia nervosa. Psychosom Med. 2015;77(9):969–981. DOI:10.1097/PSY.0000000000000247
- Zingone F, Swift GL, Card TR, Sanders DS, Ludvigsson JF, Bai JC. Psychological morbidity of celiac disease: a review of the literature. United European Gastroenterol J. 2015;3(2):136-145. DOI:10.1177/2050640614560786
- Melton SL, Knowles SR, Gwee KA, Gibson PR, Tuck CJ, Day AS. Diet Stacking – An Expanding Challenge for Gastroenterologists and Dietitians in Managing Chronic Gastrointestinal Disorders. JGH Open. 2025 Dec 9;9(12):e70314
- Lee AR, Dennis M, Lebovits J, Welstead L, Verma R, Therrien A, Lebwohl B. Dietary assessments in individuals living with coeliac disease: key considerations. J Hum Nutr Diet. 2025 Feb;38(1):e13380
- Blom JJ, Gidrewicz D, Turner J, Duerksen DR, Pinto-Sánchez MI. Diagnosis and management of celiac disease. CMAJ. 2025 Nov 10;197(38):E1258-E1265. DOI: 10.1503/cmaj.230091
- Mond JM, Hay PJ, Rodgers B, Owen C, Beumont PJ. Validity of the Eating Disorder Examination Questionnaire (EDE-Q) in screening for eating disorders in community samples. Behav Res Ther. 2004;42(5):551-567. DOI:10.1016/S0005-7967(03)
00161-X - Open Resources for Nursing. Chapter 13: Eating Disorders. In: Ernstmeyer K, Christman E, eds. Nursing: Mental Health and Community Concepts. Chippewa Valley Technical College; 2022. Accessed May 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK590029/
- Hay P. Current approach to eating disorders: a clinical update. Intern Med J. 2020;50(1):24-29. DOI:10.1111/imj.14691
- Peschel SKV, Sigrist C, Voss C, et al. Subclinical patterns of disordered eating behaviors in the daily life of adolescents and young adults from the general population. Child Adolesc Psychiatry Ment Health. 2024;18(1):69. Published 2024 Jun 6. DOI:10.1186/s13034-024-00752-w
- Reba-Harrelson L, Von Holle A, Hamer RM, Swann R, Reyes ML, Bulik CM. Patterns and prevalence of disordered eating and weight control behaviors in women ages 25-45. Eat Weight Disord. 2009;14(4):e190-e198. DOI:10.1007/BF03325116
Correspondencia: María Inés Pinto-Sanchez
Correo electrónico: pintosm@mcmaster.ca
Acta Gastroenterol Latinoam 2026;56(2):135-153
Dietary Restrictions in Celiac Disease: Differential Diagnosis Between Eating Disorders and Disordered Eating
C V Noejovich1,2 ID· N Bhola3 · J J Blom2,3 ID· M P Temprano4 ID· D Armstrong1,2,3 ID· M I Pinto-Sanchez1,2,3 ID
1McMaster University, Hamilton, ON, L8S 4K1, Canada.
2Farncombe Family Digestive Health Research Institute, Hamilton, ON, L8S 4K1, Canada.
3Hamilton Health Sciences, Hamilton, ON, L8S 4K1, Canada.
4Fundación Favaloro, Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2026;56(2):154-172
Received: 21/05/2026 / Accepted: 19/06/2026 / Published online: 30/06/2026 / https://doi.org/10.52787/agl.v56i2.653
Summary
Celiac disease requires strict adherence to a gluten-free diet, which can significantly affect eating behaviors and increase the risk of eating disorders and disordered eating. Although clinically challenging, distinguishing between these conditions is essential in the context of prescribed dietary restrictions. In this literature review, we identified an increased risk of eating disorders, particularly anorexia nervosa, in individuals with celiac disease, as well as disordered eating behaviors, including excessive restriction, food-related anxiety, and social avoidance, all of which are associated with reduced quality of life. However, current assessment tools do not adequately distinguish between pathological eating behaviors and appropriate adherence to a prescribed therapeutic diet. Although a multidisciplinary approach that includes nutritional and mental health support is recommended, evidence-based therapeutic strategies specific to celiac disease are still lacking. Overall, eating disorders in celiac disease are common and clinically relevant, highlighting the need to improve their detection and develop more appropriate diagnostic tools for both clinical practice and research.
Keywords. Celiac disease, eating disorders, disordered eating, gluten-free diet, anorexia nervosa, avoidant/restrictive food intake disorder.
Restricción alimentaria en la enfermedad celíaca: diagnóstico diferencial entre trastornos de la conducta alimentaria y alimentación desordenada
Resumen
La enfermedad celíaca requiere una adherencia estricta a la dieta libre de gluten, lo que puede afectar significativamente las conductas alimentarias y aumentar el riesgo de trastornos de la conducta alimentaria y alimentación desordenada. Si bien resulta clínicamente desafiante, diferenciar estas entidades es fundamental en el contexto de una restricción dietética prescrita. En esta revisión de la literatura, identificamos un mayor riesgo de trastornos de la conducta alimentaria , especialmente de anorexia nerviosa, en personas con enfermedad celíaca, así como conductas de alimentación desordenada, incluyendo restricción excesiva, ansiedad relacionada con los alimentos y evitación social, todas asociadas con una menor calidad de vida. Sin embargo, las herramientas de evaluación actuales no distinguen adecuadamente entre conductas alimentarias patológicas y la adherencia adecuada a una dieta terapéutica prescrita. Aunque se recomienda un abordaje multidisciplinario que incluya apoyo nutricional y de salud mental, aún faltan estrategias terapéuticas específicas basadas en evidencia para la enfermedad. En conjunto, la patología alimentaria en la enfermedad celíaca es frecuente y clínicamente relevante, lo que resalta la necesidad de mejorar su detección y desarrollar herramientas diagnósticas más apropiadas tanto para la práctica clínica como para la investigación.
Palabras claves. Enfermedad celíaca, trastornos de la conducta alimentaria, alimentación desordenada, dieta libre de gluten, anorexia nerviosa, trastorno evitativo/restrictivo de la ingesta alimentaria.
Introductión
Celiac disease (CeD) is a chronic, immune-mediated condition triggered by gluten -the primary protein complex found in wheat, barley, and rye- that develops in genetically susceptible individuals.1 It is one of the most common digestive disorders worldwide and affects approximately 1% of the world’s population.2
Treatment of CeD requires strict and lifelong adherence to a gluten-free diet (GFD), as even minimal exposure to gluten can trigger an immune response.This dietary restriction represents a sustained burden for patients; their relationship with food, eating behaviors, and food-related anxiety are key factors in treatment adherence and long-term clinical outcomes.3 The constant vigilance required to maintain adherence to the GFD may contribute to the development of eating behavior disturbances,4 including disordered eating (DE). This phenomenon must be distinguished from eating disorders (EDs), clinically defined psychiatric conditions that generally precede a diagnosis of CeD or arise from psychological, social, or environmental factors independent of this disease. (Figure 1).
Figure 1. Similarities and Differences Between Eating Disorders and Disordered Eating
EDs are psychiatric conditions characterized by persistent disturbances in eating behaviors and associated thoughts, with significant medical consequences and psychosocial impairment. The main diagnostic categories include anorexia nervosa (AN), bulimia nervosa (BN), binge-eating disorder (BED), and avoidant/restrictive food intake disorder (ARFID).5 In contrast, DE represents a spectrum of maladaptive food-related attitudes and behaviors, such as rigid dietary restriction, fasting, skipping meals, or binge eating. Although these behaviors do not meet full diagnostic criteria for an ED, they may be associated with psychological distress, nutritional compromise, and suboptimal medical management.6,7 This distinction is particularly relevant in gastrointestinal conditions such as CeD, inflammatory bowel disease (IBD), irritable bowel syndrome (IBS) and food allergies or intolerance, where medically indicated dietary restrictions may evolve into excessively restrictive eating patterns or maladaptive eating behaviors.6,7
This review summarizes the current literature on ED and DE in individuals with CeD (Table 1 and Table 2), with the aim of guiding clinical recommendations and identifying critical knowledge gaps for future research.
Table 1. Studies on Eating Disorders in Celiac Disease
Continuation Table 1. Studies on Eating Disorders in Celiac Disease
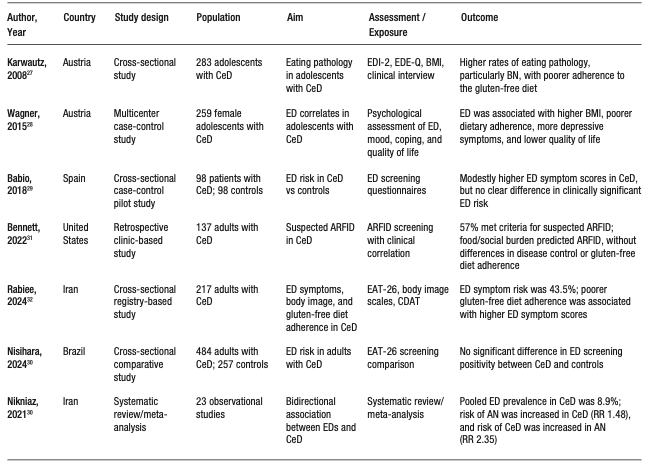
Table 2. Studies on Disordered Eating in Celiac Disease
Continuation Table 2. Studies on Disordered Eating in Celiac Disease
Eating Disorders
Eating disorders (ED) are serious psychiatric conditions characterized by persistent disturbances in eating behavior and associated thoughts or emotions, leading to significant impairment of physical and psychosocial health.8,9 The estimated lifetime prevalence of ED is approximately 1 in 7 males and 1 in 5 females by age 40, with 95% of incident cases occurring before age 25.10
This review focuses on anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), and avoidant/restrictive food intake disorder (ARFID), as this are the diagnoses most frequently addressed in research and clinical practice related to CeD (Table 3).
Anorexia nervosa (AN) is characterized by persistent restriction of energy intake leading to significantly low body weight, an intense fear of weight gain, and disturbances in body image perception, often accompanied by poor insight into illness severity and behaviors that interfere with weight restoration.8 AN includes two subtypes: the restricting type and a binge-eating/purging type, the latter involving recurrent episodes of binge eating and/or purging in addition to severe restriction.8 Complications are multisystemic, with frequent gastrointestinal involvement.11 They are accompanied by significant cognitive and emotional disturbances, high medical morbidity, and psychiatric comorbidity.8 Recent global estimates place the point prevalence of AN at approximately 43.9 cases per 100,000 individuals (0.04%) in the general population.8 Onset typically occurs in early or middle adolescence, is more common in females, and generally has a more favorable prognosis in adolescents than in adults.12 Notably, AN is associated with one of the highest mortality rates among psychiatric disorders.13
Bulimia nervosa (BN) is characterized by recurrent binge eating episodes, defined as the consumption of an objectively large amount of food accompanied by a sense of loss of control, followed by inappropriate compensatory behaviors intended to prevent weight gain, such as self-induced vomiting, misuse of laxatives, fasting, or excessive exercise.8 To meet diagnostic criteria, these behaviors must occur at least once a week over a three-months period, and self-evaluating must be disproportionately influenced by body shape and weight. When the individual has a significantly low weight, the diagnosis is reclassified as anorexia nervosa, binge-purge subtype.13 Recent estimates report a global prevalence of BN of approximately 156.85 cases per 100,000 individuals (0.16%) in the general population.14
Table 3. Most Common Eating Disorders Diagnoses in Celiac Disease and Main Symptoms75-76
Binge-eating disorder (BED) is characterized by recurrent episodes of binge eating without compensatory behaviors, occurring at least once a week for a minimum of three months.8 These episodes typically involve the rapid consumption of large quantities of food, eating in the absence of hunger, eating until a feeling of uncomfortably fullness is reached, and marked emotional distress, including feelings of shame, guilt, or depression.13 BED is approximately twice as common in women as in men and represents the most prevalent eating disorder. Its estimated global prevalence is 1.9%, reaching 2.6% in the United States, and it accounts for approximately 47% of all ED diagnoses.15,16
Avoidant/restrictive food intake disorder (ARFID) is an eating disorder characterized by persistent avoidance or restriction of food intake that leads to an inability to meet nutritional requirements. It has clinically significant consequences, including weight loss, nutritional deficiencies, dependence on supplements or nutritional support therapies, and psychosocial impairment, in the absence of body image or weight concerns.8 ARFID may manifest as highly selective eating, low appetite, sensory-based food avoidance, or restriction driven by anxiety or fear of adverse consequences, such as choking or vomiting.13 ARFID differs from disordered eating (DE), a term describing problematic eating behaviors or attitudes, such as food avoidance or dietary restriction, that may be transient or context-dependent and do not necessarily result in clinically significant nutritional, functional, or psychosocial impairment.
Population-based data from the United States indicate that individuals with eating disorders defined according to DSM-5 criteria -including AN, BN, BED and ARFID- have higher rates of concurrent psychiatric comorbidity, particularly mood disorders, anxiety disorders, substance use disorders, and personality disorders. Among these comorbidities, major depressive disorder is the most common, followed by alcohol use disorder.17
Table 3 summarizes the most common eating disorders in celiac disease
Eating Disorders in Celiac Disease
The association between eating disorders (ED) and celiac disease (CeD) varies across available studies. A meta-analysis and systematic review18 reported a combined prevalence of EDs of 8.88% in individuals with CeD, and identified a bidirectional relationship between the two conditions, with the strongest and most consistent association observed with anorexia nervosa (AN). Population-based studies, in both adult19 and pediatric cohorts20 have also demonstrated an increased risk of ED in individuals with CeD. Similarly, Lebwohl et al.21 reported an elevated risk of ED both before and after CeD diagnosis, supporting a complex bidirectional temporal relationship. Furthermore, large studies based on administrative database from the United States and Ontario suggest that individuals with CeD have a modest to substantially increased risk of ED diagnoses compared with controls, with reported increases of approximately 1.5 to 2 times, depending on the population studied and the ED subtype.22,23
Population-based cohort studies provide more specific evidence regarding the bidirectional association between CeD and AN. A Swedish national study showed that individuals with biopsy-confirmed CeD had an approximately 1.4 to 1.5 fold higher risk of developing AN compared to the general population. Conversely, individuals with a prior diagnosis of AN had an approximately 2-fold higher risk of subsequently developing CeD.24 These findings have been replicated by Hedman et al.,25reinforcing the consistency of the epidemiological link between CeD and AN.
The clinical presentation of ED in CeD is highly heterogeneous. In adults with untreated CeD, higher scores on measures of eating disorder symptoms have been reported, particularly in women, with Eating Attitudes Test (EAT-26) scores that are approximately 1.5 to 2 times higher than those observed in controls.26
In adolescents, higher rates of BN and a broader spectrum of eating disorders have been described (between 10 and 15% in some cohorts), with CeD preceding the onset of ED in most cases.27 In adolescents with CeD, the presence of comorbid EDs was associated with higher BMI, more depressive symptoms, and poorer quality of life compared to those without EDs.28 The association with a higher BMI suggests that disordered eating in this population are not limited to restrictive phenotypes with low-weight.
However, findings from case-control studies remain inconsistent. For instance, Babio et al.29 reported only modest differences in screening scores for EDs between individuals with CeD and controls, while Nisihara et al.30 found no significant difference in ED risk. More recently, ARFID has emerged as a clinically relevant phenotype in CeD, with one study reporting that more than half of adults with CeD met criteria suggestive of ARFID,31 driven primarily by food-related anxiety and social burden associated with eating.
The relationship between DE and GFD adherence also appears complex. Although one might expect restrictive phenotypes such as AN or ARFID to be associated with greater dietary rigidity and higher adherence to the GFD, Rabiee et al.,32 found that higher scores on symptoms consistent with EDs were significantly associated with lower adherence to the GFD.
Taken together, these findings suggest a higher burden of ED symptoms in subgroups of individuals with CeD, although estimates vary substantially depending on study design, the population assessed, and the measurement methods used. The most consistent evidence supports a bidirectional relationship between CeD and AN, whereas associations with other ED subtypes remain less robust.
Diagnosis and Assessment of Eating Disorders in Celiac Disease
The diagnosis of ED is primarily clinical and should be based on DSM-5-TR criteria rather than on screening instruments.8 Although ED can occur across all ages, gender, or ethnic background, adolescents and young adults are the groups at highest risk, and AN typically presents at an earlier age than BN.33
A comprehensive assessment should include evaluation of weight changes over time, patterns of food restriction or binge eating, the use of compensatory behaviors (Table 3), and attitudes associated with eating and body image, along with screening for psychiatric and medical comorbidities.8,9 The evaluation should also consider the patient’s motivation for treatment and the availability of psychosocial support.12 Brief screening tools such as the SCOFF (Table 4),34 can be useful as a first step; however, a positive result requires confirmatory diagnostic evaluation by a mental health professional, ideally a psychiatrist.13,35 Diagnostic confirmation can be supported by structured interviews such as the Eating Disorder Examination (EDE)36 and the Eating Disorder Assessment for DSM-5 (EDA-5).37 Similarly, self-administered instruments such as the Eating Disorder Inventory (EDI-3)38 can be useful for monitoring symptoms and conducting longitudinal assessment.39 Given the potential for medical instability associated with EDs, including bradycardia, hypotension, electrolyte disturbances, dehydration, or signs of malnutrition, medical risk should be systematically evaluated when an ED is suspected, with referral to higher-level care when clinically indicated.13,40
Table 4. SCOFF34 Screening of Eating Disorders in Clinical Practice
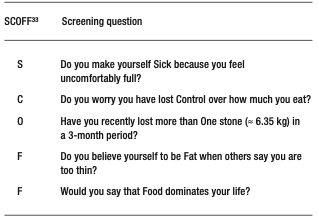
Clinical Management of Eating Disorders in Celiac Disease
The management of EDs in individuals with CeD requires a dual approach, integrating strict medical treatment of CeD with evidence-based therapeutic interventions for EDs. This overlap poses significant clinical challenges, as adherence to the GFD may inadvertently reinforce restrictive or obsessive eating patterns. Consequently, care should be provided by an integrated multidisciplinary team, with the goal of ensuring consistent messaging, minimizing unnecessary food-related fears, and clearly differentiating between medically indicated dietary restrictions and pathological restrictive behaviors driven by the ED.
As with patients without CeD, effective management of ED in CeD relies on a coordinated multidisciplinary approach, with individualized treatment based on the patient’s specific diagnosis, age, nutritional status, and medical risk. Collaboration among physicians, dietitians, and mental health professionals is essential, and early diagnosis, along with timely, evidence-based intervention, is associated with better clinical outcomes.9,13,40 In BED, the primary therapeutic goals include nutritional rehabilitation and weight restoration, combined with disorder-specific psychotherapy; in adolescents and young adults with family or caregiver support, family-based treatment is the strategy of choice.9,12,40 Cognitive-behavioral therapy (CBT) is the first-line treatment for BN, and fluoxetine may be considered as an adjunctive treatment or effective therapeutic alternative when clinically indicated.35,40 In AN, behavioral therapy (BT) and interpersonal psychotherapy have demonstrated solid efficacy, in both individual and group formats, and antidepressants may be considered in selected cases.35,40 The management of ARFID focuses on restoring adequate nutritional intake, correcting nutritional deficiencies, expanding diet variety, and addressing avoidance behaviors through behavioral interventions, exposure-based therapies, cognitive-behavioral therapy, and family-based treatments.41,42 The evidence for ARFID treatment remains more limited than for other EDs, and there is currently no universally accepted standard approach. In general, a stepped-care and coordinated model is recommended, in which treatment intensity is adjusted to the level of clinical risk, simultaneously integrating medical, nutritional, and psychological support.35,40,42,43
Disordered Eating in Celiac Disease
In CeD, strict adherence to the GFD introduces unique challenges that can significantly influence eating behaviors.4,44-46 The need for constant vigilance -including careful review of food labels, prevention of crosscontact, and management of social situations involving food- can lead to increased monitoring of food intake and food-related anxiety.4,47 Although these behaviors are adaptive and medically necessary, in some individuals they evolve into maladaptive patterns resembling DE, such as excessive restriction, behavioral rigidity, or avoidance of eating outside the home.46,48-51 Emerging evidence suggests a complex interaction between CeD and DE behaviors, with potential implications for psychological well-being and quality of life. It has been demonstrated that individuals with CeD exhibit higher rates of food neophobia, compared with non-CeD individuals -defined as fear or avoidance of new or unfamiliar foods-and of orthorexia nervosa (ON), characterized by a pathological preoccupation with consuming foods perceived as healthy, pure or “clean”. These situations involve restrictive dietary behaviors, food avoidance, emotional distress when these behaviors are violated, and potential nutritional or psychosocial impairment.49 In CeD, the distinction between AN and ON can be challenging, given that medically appropriate gluten avoidance may resemble orthorexic behaviors; clinical concern arises when dietary restriction becomes excessive, anxiety-driven, nutritionally harmful, or extends beyond what is medically necessary. Satherley et al.45 reported elevated DE symptom scores in CeD populations, including both restrictive behaviors and episodes of binge eating. Similarly, Cadenhead et al.,52 found that more than half of adolescents with CeD exhibited maladaptive eating patterns, such as rigidity, excessive preoccupation with food, and food avoidance, which were associated with a reduced quality of life.
Dietary vigilance itself appears to contribute to disease burden. Adaptive vigilance in maintaining a GFD involves proportionate and flexible behaviors that support safe disease management, whereas hypervigilance is characterized by excessive, anxiety-driven monitoring that leads to unnecessary restrictions, social impairment or a reduced quality of life. Studies on various gastrointestinal diseases, including CeD, have shown that strict dietary control is associated with increased food-related hypervigilance and reduced food-related quality of life.46-48
In specific CeD cohorts,51-53 greater adherence to the GFD has been associated with a greater perceived burden and lower quality of life, while maladaptive food attitudes assessed using tools such as the Celiac Disease Food Attitudes and Behaviors (CD-FAB) scale correlated with less favorable patient-reported outcomes.
The social implications of GFD adherence further exacerbate this burden. Lebovits et al.48 reported that 68.4% of CeD patients indicated a moderate-to-major impact of their diagnosis on dating life, including concerns about physical intimacy and discomfort when discussing dietary needs in public settings, which contributed to episodes of intentional nonadherence. Similarly, Leffler et al.50 found that adherence to a GFD negatively affected social functioning, with 44.2% of participants avoiding eating outside the home and 21.4% avoiding participation in social events. These factors may contribute to both intentional non-adherence and the development or maintenance of maladaptive eating behaviors.
Overall, current evidence suggests that, while dietary vigilance is essential for CeD management, it may also predispose a subgroup of individuals to the development of DE behaviors, with important implications for psychological well-being and quality of life.
Table 3 summarizes studies on DE behaviors in CeD.
Diagnosis and Assessment of Disordered Eating in Celiac Disease
The assessment of DE in CeD requires careful distinction between adaptive adherence to a GFD and maladaptive restrictive eating behaviors that exceed medical necessity. Because DE is not a formal diagnosis but rather a broad term that encompasses problematic eating attitudes or behaviors that may be subclinical or context-specific, evaluation should include assessment of dietary rigidity, fear of gluten exposure, food-related anxiety, psychosocial impairment, nutritional status, and the impact of eating behaviors on daily functioning. Examples of DE behaviors can be found in Table 5. Tools such as the Celiac Disease Food Attitudes and Behaviors (CD-FAB) scale may help identify maladaptive food-related cognitions and behaviors, although they do not establish a psychiatric diagnosis. It is essential to consider and rule out, when appropriate, the presence of an ED, including AN, BN, BED or ARFID, since these conditions are defined psychiatric diagnosis that require specific therapeutic approaches.
Table 5. Examples of Disordered Eating Behaviors77,78
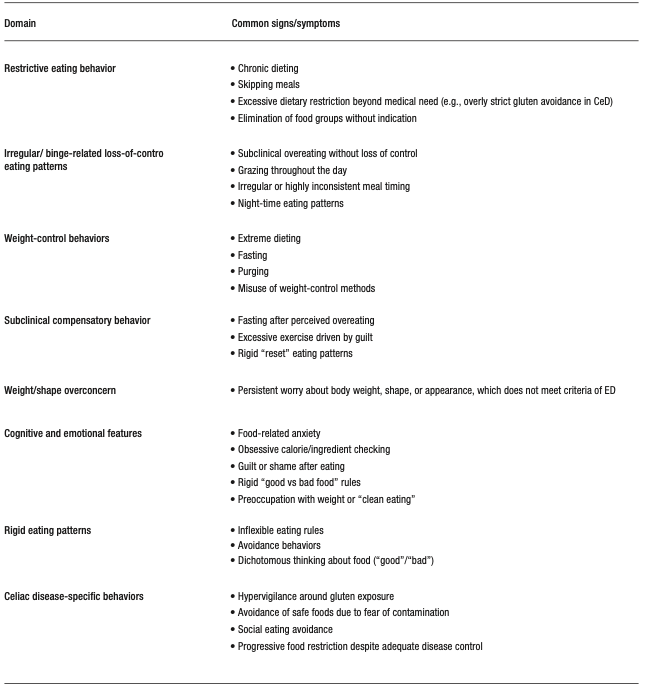
Management of Disordered Eating in Celiac Disease
Currently, there are no specific treatment guidelines for CeD that address the management of disordered eating. The available literature supports a multidisciplinary, prevention-oriented approach that integrates medical, dietary and psychological care, along with ongoing education and longitudinal monitoring.52,54,55 Where comprehensive multidisciplinary care is unavailable, a minimal pragmatic care model should include a treating physician (gastroenterologist or primary care physician) responsible for clinical evaluation and medical monitoring, a dietitian with experience in CeD to guide safe and nutritionally adequate GFD management, and referral to a mental health professional, when available, upon suspicion of underlying psychological factors or an ED, with escalation to specialized care based on clinical severity and medical risk.49,50 Given that the cornerstone of CeD management is lifelong adherence to a GFD, clinicians must carefully balance the need for strict gluten avoidance with the risk of reinforcing maladaptive eating patterns, and to prevent progression to a formal ED.56,57 In CeD, DE may arise from symptom-driven food restriction, hypervigilance defined as monitoring, worry or excessive or disproportionate avoidance behaviors related to the risk of accidental gluten ingestion or cross-contact, beyond what is reasonably required for safe disease management, or fear of adverse outcomes, all of which are amplified by the demands of strict dietary adherence.44,58 In this context, clinical follow-up should include structured and repeated assessments of eating patterns and their context, avoiding the automatic assumption that increasing restriction reflects appropriate adherence or, conversely, prematurely labeling it as psychiatric pathology.47,56
Clinical assessments should extend beyond GFD adherence to assess patterns suggestive of maladapted eating, including meal skipping, fasting to avoid symptoms, a progressive reduction in dietary variety, avoidance of safe foods, fear of eating outside the home, excessive reliance on foods prepared exclusively by the patient and persistent preoccupation with food. Additional concerning features include unintentional weight loss, body image disturbance, compensatory behaviors (e.g., purging or laxative use) and persistent gastrointestinal symptoms despite escalating restriction.56,58
There is very limited information on the routine implementation of formal screening tools for ED or DE in CeD clinics and currently there are no clinical guidelines recommending universal standardized screening for ED/DE in all CeD patients. However, selected screening instruments may support case identification in higher-risk individuals, including general ED tools such as the Eating Disorder Screen for Primary Care (ESP),59 the SCOFF questionnaire,34 as well as CeD-specific instruments such as the Celiac Disease Food Attitudes and Behaviors Scale (CD-FAB),60 which may help identify maladaptive food-related attitudes and behaviors.
Nutritional management should be carried out by dietitians with expertise in both CeD and EDs, with the goal of maintaining strict gluten exclusion while minimizing unnecessary restrictions. This includes promoting dietary variety within the GFD, clarifying the distinction between medically-required and avoidant restrictions and addressing food-related fears such as cross-contact. Psychological interventions are a core component of treatment and should target maladaptive cognition and behaviors related to food, food safety and body image. In this context, evidence-based approaches including cognitive-behavioral therapy (CBT) and family-based treatment can be adapted to address features that overlap with conditions such as ARFID and AN.
Developmental considerations are also important, as maladaptive eating behaviors often emerge during adolescence.61 In individuals with CeD, early risk factors such as dissatisfaction with body weight, symptoms of anxiety or depression, and family dynamics surrounding meals, may interact with the chronic demands of a GFD, perpetuating or exacerbating DE behaviors into adulthood.45,62 When DE behaviors are identified, clinicians should assess the patient’s medical stability and initiate early referral to mental health professionals, ideally those with expertise in EDs and familiarity with gastrointestinal conditions.56 Finally, it is essential to maintain consistent and coordinated messaging across disciplines to avoid reinforcing fear-driven eating patterns or excessive restrictions.
Nutritional Challenges in the Management of Eating Disorders and Disordered Eating in Celiac Disease
The management of EDs, particularly AN, BN and ARFID in individuals with medically prescribed restrictive diets, such as those with CeD, presents a unique therapeutic paradox. Standard EDs treatment aims to reduce rigid dietary rules, challenge food avoidance and restore flexibility in the relationship with food, whereas CeD requires strict and lifelong adherence to a gluten-free diet (GFD), creating an inherent tension between psychological recovery and medical necessity.26,63 This difficulty is especially relevant in restrictive phenotypes of EDs, in which the GFD may inadvertently reinforce restrictive cognitions or even become integrated into the disorder as a socially acceptable form of avoidance.64,65
From a nutritional perspective, maintaining a strict GFD while working to normalize eating patterns is inherently complex. A GFD requires the complete exclusion of wheat, rye, barley and related grains, as well as constant vigilance regarding hidden gluten sources and cross-contact during food processing, storage, and preparation. Without appropriate guidance, this necessary vigilance may evolve into excessive dietary restriction. Dietary management should therefore emphasize nutritionally adequate gluten-free substitutions, including whole grains and balanced meal planning to support sufficient caloric and nutrient intake.
This is particularly important given the nutritional limitations of many commercial gluten-free products, which are often not fortified with key micronutrients such as iron, folate, thiamine, riboflavin, and niacin. In a study by Jamieson et al.,66 gluten-free staple products contained 1.3 times more fat and significantly lower levels of iron (-55%), folate (-44%), and protein (-36%) compared with gluten-containing counterparts. Variability in the content and composition of fiber -particularly fermentable fiber- may contribute to the persistence of gastrointestinal symptoms and negatively affect psychological well-being in patients with CeD.67
This is exacerbated in patients with coexisting EDs, in whom insufficient intake, elimination of food groups, binge-purge behaviors and erratic eating patterns can exacerbate micronutrient deficiencies commonly seen in both conditions, such as iron, B-complex vitamins, and essential fatty acids.65,68 Altered eating behaviors may also contribute to gut microbiome dysbiosis, potentially worsening gastrointestinal symptoms and complicating dietary adherence.69 In non-restrictive ED phenotypes such as BN and BED, episodes of uncontrolled intake may increase the risk of inadvertent gluten exposure, particularly when gluten-free options are limited.64,68
DE in CeD presents overlapping but distinct nutritional challenges. Unlike formal ED, DE in CeD is often driven by symptom-related anxiety, fear of gluten exposure or excessive dietary vigilance, rather than body image concerns. Patients may progressively eliminate foods beyond what is medically necessary, reducing dietary diversity and increasing the risk of nutritional inadequacy despite the adherence to GFD.65,66 Hypervigilance around cross-contact and reliance to a GFD on a narrow repertoire of perceived “safe” foods may further impair quality of life and reinforce avoidance behaviors.63,65,70 Access to a dietitian with CeD expertise can help reduce the risk of diet stacking, whereby patients progressively adopt multiple overlapping and unnecessary dietary restrictions beyond the GFD, increasing food-related anxiety, nutritional compromise, and psychosocial burden.71
Weight changes following the onset of a GFD can further complicate management. Weight restoration in previously malnourished individuals or weight gain associated with improved absorption and increased availability of processed gluten-free foods may contribute to body image concerns, triggering DE behaviors or exacerbating pre-existing ED, particularly in adolescents and young adults.63,70 It is necessary to use standardized, evidence-based educational tools, including cross-contact checklists, which may help reduce unnecessary fear, improve consistency in counseling and support a better understanding of gluten exposure risk.72 An example of a cross-contact checklist was published in a recent review.73
From a practical perspective, a hierarchy of nutritional goals in the management of DE begins with nutritional adequacy, prioritizing the restoration of consistent and sufficient energy intake, given that insufficient or erratic eating can worsen gastrointestinal symptoms, increase food-related anxiety and reinforce restrictive behaviors. Once adequate intake is established, the focus should shift to nutritional balance, ensuring meals that provide sufficient carbohydrates, protein and fat to promote satiety, nutritional adequacy, and more predictable digestive function. The next step is dietary variety, promoting a gradual expansion beyond a limited range of foods considered “safe”, with the goal of improving dietary diversity, nutritional quality, and confidence in eating. Only once these foundations are established should the reintroduction of specific feared or avoided foods be addressed, using a gradual and structured approach to dietary rehabilitation (Figure 2). This stepwise model aligns with established principles of nutritional rehabilitation in eating disorders , emphasizing the restoration of adequate intake, balanced nutrition, dietary variety and gradual reintroduction of feared foods.
Figure 2. Stepwise Recommendations for Dietary Rehabilitation in Patients with Disordered Eating
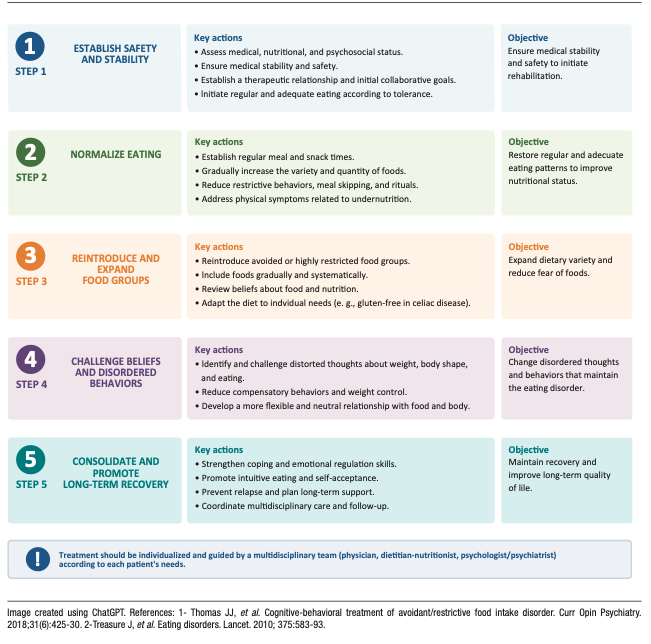
Recommendations for the Clinical Management of Eating Disorders and Disordered Eating in Celiac
Disease
This section provides practical guidance for clinicians managing ED and DE in individuals with CeD, with an emphasis on clinical decision-making and the delineation of roles within the care team.
In patients with restrictive eating, food-related anxiety, weight change or distress associated with the GFD, the first clinical task is to determine whether these manifestations correspond to a DE pattern or an ED requiring specialized mental health evaluation. Distinguishing between adaptive adherence to the GFD and patterns of DE or a formal ED can be challenging, as medically necessary restriction may overlap with maladaptive or pathological behaviors. Brief tools such as the SCOFF questionnaire34 or the Eating Disorder Examination Questionnaire (EDE-Q)74 support early identification in clinical settings. Severe restrictions with low weight, fear of weight gain, binge eating, compensatory behaviors or marked body image disturbance suggest an ED, whereas hypervigilance, rigid safety behaviors or progressive narrowing of food choices may reflect DE.
When an ED is suspected, the role of the physician is to recognize warning signs, assess medical stability, and facilitate a timely referral to mental health services or specialized ED programs. ED requires specialized psychiatric management; nutrition-focused interventions alone may be insufficient or they may inadvertently reinforce maladaptive behaviors. For both of these reasons, early referral is essential.
In patients with DE not meeting ED criteria, physicians and dietitians play a more active role in management. Treatment should focus on maintaining strict gluten exclusion while minimizing unnecessary dietary restriction, supporting nutritional adequacy and addressing maladaptive food-related beliefs. When patients are reluctant to engage with mental health services, clinicians should maintain longitudinal follow-up, document clinical concerns, and reconsider referral using clear, nonjudgmental language focused on functionality, safety, and quality of life.
Within this framework, several practical recommendations can guide management:
1. Assess the severity and context of altered eating behaviors to differentiate DE from ED.
2. Refer patients early when there are features consistent with an eating disorder, significant psychological distress, or nutritional risk.
3. Promote multidisciplinary collaboration with dietitians and mental health professionals experienced in both CeD and EDs.
4. Reinforce evidence-based education on GFD to prevent excessive or unnecessary restrictions.
5. Acknowledge the psychological burden of dietary vigilance, particularly in social contexts and situations of food uncertainty.
6. Conduct longitudinal monitoring of eating behaviors, nutritional status, and psychosocial impact.
Overall, management should be individualized and multidisciplinary, with a clear delineation of roles across specialties.
Figure 3 presents a summary of the diagnosis and management of EDs and DE in CeD.
Addressing Hypervigilance in Celiac Disease
Hypervigilance regarding gluten exposure warrants particular attention in the management of CeD.
While patients must develop practical skills to maintain a GFD -including reading labels, preventing cross-contact, and making safe food choices- in some individuals these behaviors may become excessively rigid or fear-driven.
In such cases, patient education is a central component of management.
Clear, evidence-based counseling from the clinical team or a dietitian specializing in CeD can help correct misconceptions about gluten exposure risk, clarify high-risk versus low-risk scenarios, and reduce uncertainty around food labeling, cross-contact, and safe practices when eating out.
The use of standardized educational tools, practical checklists, and consistent messaging among different healthcare professionals can help reduce unnecessary fears and prevent conflicting recommendations that may exacerbate anxiety.30-32
Behavioral strategies can also be helpful, particularly when hypervigilance leads to progressive restriction or psychosocial impairment.
Gradual reintroduction of unnecessarily avoided but safe foods, expansion of dietary variety and supported exposure to low-risk social eating situations can help rebuild confidence and reduce reliance on a narrow repertoire of foods perceived as “safe”.
The goal is not to reduce adherence to the GFD, but to promote proportionate vigilance which is maintaining medical safety while minimizing unnecessary restrictions, food-related anxiety and impaired quality of life.
Figure 3 summarizes a stepwise approach to the screening, diagnosis, and management of eating disorders and disordered eating in celiac disease.
Figure 3. Screening, Diagnosis and Management of Eating Disorders and Disordered Eating in Celiac Disease
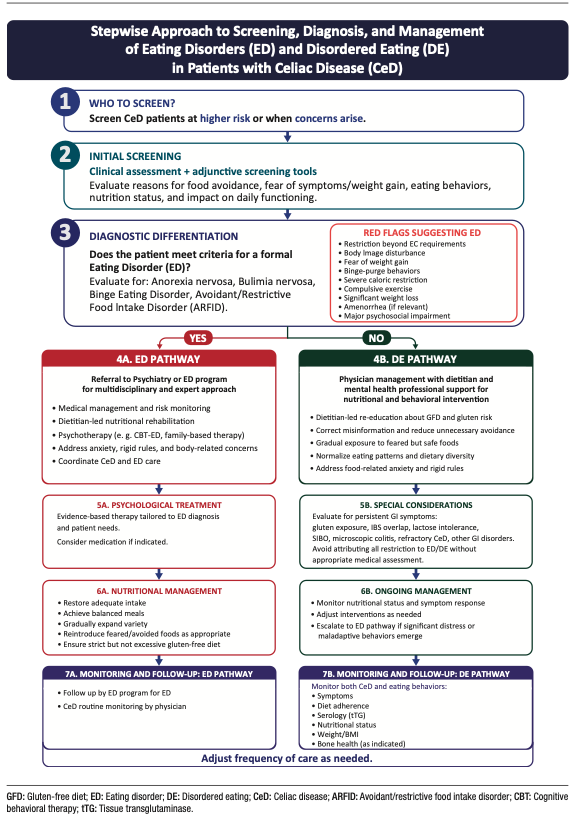
Discussion
The intersection between CeD, maladaptive eating behaviors and EDs represent an important and under-recognized challenge in gastroenterology. These conditions may mimic, obscure or exacerbate one another, as they share overlapping features including weight changes, abdominal pain, altered bowel habits, fatigue, micronutrient deficiencies, and malnutrition.8 (Figure 1). As a result, distinguishing between ongoing intestinal disease activity, poor dietary adherence and coexisting DE or EDs can be particularly difficult in patients with persistent symptoms or nutritional compromise despite strict dietary adherence.
This complexity is heightened by the fact that CeD treatment is inherently dietary. While strict adherence to GFD is essential, the required vigilance may contribute to hypervigilance, rigidity and food-related anxiety in susceptible individuals, potentially evolving into maladaptive eating patterns. Conversely, pre-existing EDs may interfere with treatment adherence, nutritional rehabilitation and the clinical interpretation of symptoms. These dynamics underscore the importance of distinguishing adaptive dietary management from pathological restriction as a core component of CeD care. In this context, EDs and DE should be recognized as clinically relevant factors influencing adherence, symptom persistence, nutritional risk and quality of life, justifying a multidisciplinary approach involving gastroenterologists, dietitians, and mental health professionals.
Psychosocial factors appear to play a key role in this interaction. A higher burden of symptoms consistent with EDs has been associated with depressive symptoms, lower quality of life, greater social burden, and body dissatisfaction.28,30-32 These findings support a biopsychosocial framework, although the directionality of these relationships remains unclear, as psychosocial distress may act as both a contributing factor or be a consequence of maladaptive eating behaviors. Prospective longitudinal studies are needed to clarify temporal relationships, identify predictors of progression from DE to formal ED, and determine whether targeted psychosocial interventions can improve clinical and quality-of-life outcomes in individuals with CeD.
Several important gaps in knowledge remain. First, there is limited guidance on how to adapt nutritional interventions for CeD patients with coexisting DE or ED. Standard dietary counseling, delivered in isolation, may be insufficient or may inadvertently reinforce restrictive or fear-driven behaviors. Second, there is a lack of treatment-focused evidence. Most of the available studies are cross-sectional or observational and do not evaluate the effectiveness of integrated care models. It remains unclear whether standard ED treatments require modifications in the context of CeD, or what the best strategy is for coordinating gastrointestinal, nutritional and psychiatric care.
Third, there is a lack of validated tools specifically designed to distinguish maladaptive eating behaviors from medically necessary dietary restriction. Existing instruments (e.g., EAT-26, SCOFF) were developed for the general populations and may have limited specificity in conditions requiring therapeutic dietary modification, such as CeD, food allergy, inflammatory bowel disease, eosinophilic gastrointestinal disorders or irritable bowel syndrome managed with elimination diets. Although condition-specific tools, such as the Celiac Disease Food Attitudes and Behaviors (CD-FAB) scale, show potential for identifying maladaptive food-related cognitions and behaviors in CeD, further validation and broader clinical implementation are needed.51,60
Finally, the role of social determinants of health (SDOH), including food access, health literacy and social support, remains underexplored, despite their likely influence on vulnerability to DE in CeD.
Future research should prioritize longitudinal studies that clarify the temporal relationships between CeD, DE and ED, as well as intervention trials that evaluate multidisciplinary and integrated care models. The development of assessment tools specific to CeD and the incorporation of conceptual frameworks based on the SDOH will be critical to improving both clinical care and research in this population.
Intellectual property. The authors declare that the data, figures and tables in this article are original and were carried out at their institutions.
Funding. David Armstrong is supported by the Douglas Family Chair in Nutrition Research. MIPS is supported by the Farncombe Family Digestive Health Research Institute Nutrition Initiative.
Conflict of interest. María Inés Pinto-Sanchez received research funding from Celiac Canada, Takeda and Provention Bio and an educational grant from Takeda. MIPS is member of the Scientific Medical Advisory Board of Celiac Canada.
Copyright
© 2026 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Noejovich C V, Bhola N, Blom J J et al. Dietary Restrictions in Celiac Disease: Differential Diagnosis Between Eating Disorders and Disordered Eating Acta Gastroenterol Latinoam. 2026;56(2):154-172. https://doi.org/10.52787/agl.v56i2.653
References
- Catassi C, Verdu EF, Bai JC, Lionetti E. Coeliac disease. Lancet. 2022;399(10344):2413-2426. DOI:10.1016/S0140-6736(22)
00794-2 - Singh P, Arora A, Strand TA, et al. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16(6):823-36.e2. DOI:10.1016/j.cgh.2017.06.037
- Hallert C, Grännö C, Hultén S, et al. Living with coeliac disease: controlled study of the burden of illness. Scand J Gastroenterol. 2002;37(1):39-42. DOI:10.1080/003655202753387338
- de Rosa A, Troncone A, Vacca M, Ciacci C. Characteristics and quality of illness behavior in celiac disease. Psychosomatics. 2004;45(4):336-342. DOI:10.1176/appi.psy.45.4.336
- American Psychiatric Association. What are eating disorders? Psychiatry.org. Accessed March 17, 2026. https://www.psychiatry.org/patients-families/eating-disorders/what-are-eating-disorders
- Peters JE, Basnayake C, Hebbard GS, Salzberg MR, Kamm MA. Prevalence of disordered eating in adults with gastrointestinal disorders: A systematic review. Neurogastroenterology and Motil. 2022;34(8):e14278. DOI:10.1111/nmo.14278
- Staller K, Abber SR, Burton Murray H. The intersection between eating disorders and gastrointestinal disorders: a narrative review and practical guide. Lancet Gastroenterol Hepatol. 2023;8(6):565-578. DOI:10.1016/S2468-1253(22)00351-X
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, text rev (DSM-5-TR). Washington, DC: American Psychiatric Association Publishing; 2022.
- Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. 2020;395(10227):899-911. DOI:10.1016/S0140-6736(20)300
59-3 - Ward ZJ, Bleich SN, Cradock AL, et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. JAMA Netw Open. 2019;2(10):e1912925. DOI:10.1001/jamanetworkopen.2019.
12925 - Schalla MA, Stengel A. Gastrointestinal alterations in anorexia nervosa – A systematic review. Eur Eat Disord Rev. 2019;27(5):447-461. DOI:10.1002/erv.2679
- Zipfel S, Giel KE, Bulik CM, Hay P, Schmidt U. Anorexia nervosa: aetiology, assessment, and treatment. Lancet Psychiatry. 2015;2(12):1099-1111. DOI:10.1016/S2215-0366(15)
00356-9 - Academy for Eating Disorders (AED) Medical Care Standards Committee. Eating Disorders: A Guide to Medical Care. 4th ed. Reston, VA: Academy for Eating Disorders;2021.
- Shen Y, Chen B, Zhang H, Shen W, Wu C, Jiang L. Global, regional, and national burden of eating disorders in 204 countries and territories, 1990-2021: findings from the Global Burden of Disease Study 2021. J Eat Disord. 2025;13(1):290. Published 2025 Dec 20. DOI:10.1186/s40337-025-01492-8
- Mars JA, Iqbal A, Rehman A. Binge Eating Disorder. In: StatPearls. StatPearls Publishing; 2026. Updated August 11, 2024. Accessed May 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK551700/
- Santomauro DF, Melen S, Mitchison D, Vos T, Whiteford H, Ferrari AJ. The hidden burden of eating disorders: an extension of estimates from the Global Burden of Disease Study 2019. Lancet Psychiatry. 2021;8(4):320-328. DOI:10.1016/S2215-0366
(21)00040-7 - Udo T, Grilo CM. Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States.Int J Eat Disord. 2019;52(1):42-50. DOI:10.1002/eat.23004
- Nikniaz Z, Beheshti S, Abbasalizad Farhangi M, Nikniaz L. A systematic review and meta-analysis of the prevalence and odds of eating disorders in patients with celiac disease and vice-versa. Int J Eat Disord. 2021;54(9):1563-1574. DOI:10.1002/eat.23561
- Hansen S, Osler M, Thysen SM, Rumessen JJ, Linneberg A, Kårhus LL. Celiac disease and risk of neuropsychiatric disorders: A nationwide cohort study. Acta Psychiatr Scand. 2023;148(1):60-70. DOI:10.1111/acps.13554
- Butwicka A, Lichtenstein P, Frisén L, Almqvist C, Larsson H, Ludvigsson JF. Celiac Disease Is Associated with Childhood Psychiatric Disorders: A Population-Based Study. J Pediatr. 2017;
184:87-93.e1. DOI:10.1016/j.jpeds.2017.01.043 - Lebwohl B, Haggård L, Emilsson L, et al. Psychiatric Disorders in Patients with a Diagnosis of Celiac Disease During Childhood From 1973 to 2016. Clin Gastroenterol Hepatol. 2021;19(10):2093-2101.e13. DOI:10.1016/j.cgh.2020.08.018
- Alkhayyat M, Qapaja T, Aggarwal M, et al. Epidemiology and risk of psychiatric disorders among patients with celiac disease: A population-based national study. J Gastroenterol Hepatol. 2021;36(8):2165-2170. DOI:10.1111/jgh.15437
- Subramanian L, Coo H, Jane A, et al. Celiac Disease and Inflammatory Bowel Disease Are Associated with Increased Risk of Eating Disorders: An Ontario Health Administrative Database Study. Clin Transl Gastroenterol. 2024;15(5):e00700. Published 2024 May 1. DOI:10.14309/ctg.0000000000000700
- Mårild K, Størdal K, Bulik CM, et al. Celiac Disease and Anorexia Nervosa: A Nationwide Study. Pediatrics. 2017;139(5):
e20164367. DOI:10.1542/peds.2016-4367 - Hedman A, Breithaupt L, Hübel C, et al. Bidirectional relationship between eating disorders and autoimmune diseases. J Child Psychol Psychiatry. 2019;60(7):803-812. DOI:10.1111/jcpp.12958
- Passananti V, Siniscalchi M, Zingone F, et al. Prevalence of eating disorders in adults with celiac disease. Gastroenterol Res Pract. 2013;2013:491657. DOI:10.1155/2013/491657
- Karwautz A, Wagner G, Berger G, Sinnreich U, Grylli V, Huber WD. Eating pathology in adolescents with celiac disease. Psychosomatics. 2008;49(5):399-406. DOI:10.1176/appi.psy.49.5.399
- Wagner G, Zeiler M, Berger G, et al. Eating Disorders in Adolescents with Celiac Disease: Influence of Personality Characteristics and Coping. Eur Eat Disord Rev. 2015;23(5):361-370. DOI:10.1002/erv.2376
- Babio N, Alcázar M, Castillejo G, et al. Risk of Eating Disorders in Patients With Celiac Disease. J Pediatr Gastroenterol Nutr. 2018;66(1):53-57. DOI:10.1097/MPG.0000000000001648
- Nisihara R, Techy ACM, Staichok C, et al. Prevalence of eating disorders in patients with celiac disease: a comparative study with healthy individuals. Rev Assoc Med Bras (1992). 2024;70(1):e20231090. Published 2024 Mar 15. DOI:10.1590/
1806-9282.20231090 - Bennett A, Bery A, Esposito P, Zickgraf H, Adams DW. Avoidant/Restrictive Food Intake Disorder Characteristics and Prevalence in Adult Celiac Disease Patients. Gastro Hep Adv. 2022;1(3):321-327. Published 2022 Mar 30. DOI:10.1016/j.gastha.2022.01.002
- Rabiee R, Mahdavi R, Shirmohammadi M, Nikniaz Z. Eating disorders, body image dissatisfaction and their association with gluten-free diet adherence among patients with celiac disease. BMC Nutr. 2024;10(1):100. Published 2024 Jul 18. DOI:10.1186/s40795-024-00910-5
- Litmanen J, Fröjd S, Marttunen M, Isomaa R, Kaltiala-Heino R. Are eating disorders and their symptoms increasing in prevalence among adolescent population? Nord J Psychiatry. 2017;71(1):61-66. DOI:10.1080/08039488.2016.1224272
- Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. 1999;319(7223):1467-1468. DOI:10.1136/bmj.319.7223.1467
- National Institute for Health and Care Excellence. Eating disorders: recognition and treatment (NG69). NICE. Published May 23, 2017. Exceptional surveillance updated 2024. Accessed March 17, 2026. https://www.nice.org.uk/guidance/ng69
- Fairburn CG, Cooper Z, O’Connor ME. Eating Disorder Examination. Edition 17.0D. CBT-E website. Published January 2014. Accessed May 14, 2026. https://www.cbte.co/for-professionals/measures/
- Sysko R, Glasofer DR, Hildebrandt T, et al. The eating disorder assessment for DSM-5 (EDA-5): development and validation of a structured interview for feeding and eating disorders. Int J Eat Disord. 2015;48(5):452-463. DOI:10.1002/eat.22388
- Garner DM. Eating Disorder Inventory-3: Professional Manual. Psychological Assessment Resources; 2004.
- Schaefer LM, Crosby RD, Machado PPP. A systematic review
of instruments for the assessment of eating disorders among adults. Curr Opin Psychiatry. 2021;34(6):543-562. DOI:10.10
97/YCO.0000000000000746 - Crone C, Fochtmann LJ, Attia E, et al. The American Psychiatric Association practice guideline for the treatment of patients with eating disorders. Am J Psychiatry. 2023;180(2):167-171. DOI:10.1176/appi.ajp.23180001
- Kambanis PE, Thomas JJ. Assessment and Treatment of Avoidant/Restrictive Food Intake Disorder. Current Psychiatry Reports. 2023;25(2):53-64. DOI:10.1007/s11920-022-01404-6
- Ramirez Z, Gunturu S. Avoidant Restrictive Food Intake Disorder. In: StatPearls. StatPearls Publishing; 2024. Updated May 1, 2024.
- Di Cara M, Rizzo C, Corallo F, et al. Avoidant Restrictive Food Intake Disorder: A Narrative Review of Types and Characteristics of Therapeutic Interventions.Children (Basel). 2023;10(8):1297. Published 2023 Jul 28. DOI:10.3390/children10081297
- Coburn S, Germone M, McGarva J, Taft T. Psychological Considerations for Food Intolerances: Celiac Sprue, Eosinophilic Esophagitis, and Non-Celiac Gluten Sensitivity. Gastroenterol Clin North Am. 2022;51(4):753-764. DOI:10.1016/j.gtc.2022.07.003
- Satherley RM, Higgs S, Howard R. Disordered eating patterns in coeliac disease: a framework analysis. J Hum Nutr Diet. 2017;30(6):724-736. DOI:10.1111/jhn.12475
- Simons M, McGarva J, Doerfler B, et al. Food-related quality of life driven by hypervigilance and anxiety around eating in organic gastrointestinal conditions. J Hum Nutr Diet. 2024;37(6):1505-1515. DOI:10.1111/jhn.13358
- Lee AR, Zybert P, Chen Z, et al. Food avoidance beyond the gluten-free diet and the association with quality of life and eating attitudes and behaviors in adults with celiac disease. Nutrients. 2024;16(19):3411. DOI:10.3390/nu16193411
- Lebovits J, Lee AR, Ciaccio EJ, et al. Impact of Celiac Disease on Dating. Dig Dis Sci. 2022;67(11):5158-5167. DOI:10.1007/s10620-022-07548-y
- Zysk W, Glabska D, Guzek D. Food Neophobia in Celiac Disease and Other Gluten-Free Diet Individuals. Nutrients. 2019;11(8):
1762. Published 2019 Jul 31. DOI:10.3390/nu11081762 - Leffler DA, Dennis M, Edwards George JB, Kelly CP. The interaction between eating disorders and celiac disease: an exploration of 10 cases. Eur J Gastroenterol Hepatol. 2007;19(3):251-255. DOI:10.1097/MEG.0b013e328012db37
- Gholmie Y, Lee AR, Satherley RM, et al. Maladaptive Food
Attitudes and Behaviors in Individuals with Celiac Disease and Their Association with Quality of Life. Dig Dis Sci. 2023;68(7):2899-2907. DOI:10.1007/s10620-023-07912-6 - Cadenhead JW, Lee AR, Nguyen TTT, Lebwohl B, Green PHR, Wolf RL. Dietary Adherence to Recommendations among a Cohort of Adults and Teens with Celiac Disease Maintaining a Gluten-Free Diet Compared to a Nationally Representative Sample: A Cross-Sectional Study. Nutrients. 2024;16(18):3067. Published 2024 Sep 11. DOI:10.3390/nu16183067
- Wolf RL, Lebwohl B, Lee AR, et al. Hypervigilance to a Gluten-Free Diet and Decreased Quality of Life in Teenagers and Adults with Celiac Disease. Dig Dis Sci. 2018;63(6):1438-1448. DOI:10.1007/s10620-018-4936-4
- Rajani S, Sawyer-Bennett J, Shirton L, et al. Patient and parent
satisfaction with a dietitian- and nurse- led celiac disease clinic for children at the Stollery Children’s Hospital, Edmonton, Alberta. Can J Gastroenterol. 2013;27(8):463-466. DOI:
10.1155/2013/537160 - Mulder CJJ, Elli L, Lebwohl B, et al. Follow-Up of Celiac Disease in Adults: «When, What, Who, and Where». Nutrients. 2023;15
(9):2048. Published 2023 Apr 24. DOI:10.3390/nu15092048 - Riehl ME, Scarlata K. Understanding disordered eating risks in patients with gastrointestinal conditions. J Acad Nutr Diet. 2022;122(3):491-499. DOI:10.1016/j.jand.2021.03.001
- Ciao AC, Loth K, Neumark-Sztainer D. Preventing eating disorder pathology: common and unique features of successful eating disorders prevention programs. Curr Psychiatry Rep. 2014;16(7):453. DOI:10.1007/s11920-014-0453-0
- Quick VM, Byrd-Bredbenner C, Neumark-Sztainer D. Chronic illness and disordered eating: a discussion of the literature. Adv Nutr. 2013;4(3):277-286. DOI:10.3945/an.112.003608
- Cotton MA, Ball C, Robinson P. Four simple questions can help screen for eating disorders. J Gen Intern Med. 2003;18(1):53-56. DOI:10.1046/j.1525-1497.2003.20374.x
- Satherley RM, Howard R, Higgs S. Development and validation of the Coeliac Disease Food Attitudes and Behaviours Scale. Gastroenterol Res Pract. 2018;2018:6930269. DOI:10.1155/2018/
6930269 - Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27:281-295. DOI:10.1038/s41380-021-01161-7
- Rowen K, Solomon P, Tebbett-Mock A. Psychosocial predictors of disordered eating in adolescents with celiac disease: a cross-sectional study. Child Health Care. Published online 2026.
DOI:10.1080/02739615.2026.2626386 - Lee AR, Lebwohl B, Lebovits J, Wolf RL, Ciaccio EJ, Green PHR. Factors associated with maladaptive eating behaviors, social anxiety, and quality of life in adults with celiac disease. Nutrients. 2021;13(12):4494. DOI:10.3390/nu13124494
- Wei Y, Wang Y, Yuan Y, Chen J. Celiac disease, gluten-free diet, and eating disorders: from bench to bedside. Foods. 2025;14(1):74. DOI:10.3390/foods14010074
- Bennett A, Bery A, Esposito P, Zickgraf H, Adams DW. Avoidant/restrictive food intake disorder characteristics and prevalence in adult celiac disease patients. Gastro Hep Adv. 2022;1(3):
321-327. DOI:10.1016/j.gastha.2022.01.002 - Jamieson JA, Weir M, Gougeon L. Canadian packaged gluten-free foods are less nutritious than their regular gluten-containing counterparts. PeerJ. 2018;6:e5875. DOI:10.7717/peerj.5875
- Roncoroni L, Bascuñán KA, Doneda L, et al. A low FODMAP gluten-free diet improves functional gastrointestinal disorders and overall mental health of celiac disease patients: a randomized controlled trial. Nutrients. 2018;10(8):1023. DOI:10.3390/nu10081023
- Kaul R, Jansson-Knodell C, Simons ML, Weekley K, Gardinier D, Rubio-Tapia A. Avoidant/restrictive food intake disorder in celiac disease. Nutrients. 2025;17:3197. DOI:10.3390/nu17203197
- Kleiman SC, Watson HJ, Bulik-Sullivan EC, et al. The intestinal microbiota in anorexia nervosa. Psychosom Med. 2015;77(9):969–981. DOI:10.1097/PSY.0000000000000247
- Zingone F, Swift GL, Card TR, Sanders DS, Ludvigsson JF, Bai JC. Psychological morbidity of celiac disease: a review of the literature. United European Gastroenterol J. 2015;3(2):136-145. DOI:10.1177/2050640614560786
- Melton SL, Knowles SR, Gwee KA, Gibson PR, Tuck CJ, Day AS. Diet Stacking – An Expanding Challenge for Gastroenterologists and Dietitians in Managing Chronic Gastrointestinal Disorders. JGH Open. 2025 Dec 9;9(12):e70314
- Lee AR, Dennis M, Lebovits J, Welstead L, Verma R, Therrien A, Lebwohl B. Dietary assessments in individuals living with coeliac disease: key considerations. J Hum Nutr Diet. 2025 Feb;38(1):e13380
- Blom JJ, Gidrewicz D, Turner J, Duerksen DR, Pinto-Sánchez MI. Diagnosis and management of celiac disease. CMAJ. 2025 Nov 10;197(38):E1258-E1265. DOI: 10.1503/cmaj.230091
- Mond JM, Hay PJ, Rodgers B, Owen C, Beumont PJ. Validity of the Eating Disorder Examination Questionnaire (EDE-Q) in screening for eating disorders in community samples. Behav Res Ther. 2004;42(5):551-567. DOI:10.1016/S0005-7967(03)
00161-X - Open Resources for Nursing. Chapter 13: Eating Disorders. In: Ernstmeyer K, Christman E, eds. Nursing: Mental Health and Community Concepts. Chippewa Valley Technical College; 2022. Accessed May 14, 2026. https://www.ncbi.nlm.nih.gov/books/NBK590029/
- Hay P. Current approach to eating disorders: a clinical update. Intern Med J. 2020;50(1):24-29. DOI:10.1111/imj.14691
- Peschel SKV, Sigrist C, Voss C, et al. Subclinical patterns of disordered eating behaviors in the daily life of adolescents and young adults from the general population. Child Adolesc Psychiatry Ment Health. 2024;18(1):69. Published 2024 Jun 6. DOI:10.1186/s13034-024-00752-w
- Reba-Harrelson L, Von Holle A, Hamer RM, Swann R, Reyes ML, Bulik CM. Patterns and prevalence of disordered eating and weight control behaviors in women ages 25-45. Eat Weight Disord. 2009;14(4):e190-e198. DOI:10.1007/BF03325116
Correspondence: María Inés Pinto-Sanchez
Email: pintosm@mcmaster.ca
Acta Gastroenterol Latinoam 2026;56(2):154-172