
Victoria Veloso, Daniela Chiodi, Nelia Hernández
Departament of Gastroenterology and Hepatology, Clinic Hospital. Montevideo, Uruguay.
Acta Gastroenterol Latinoam 2020;50(3):335-340
Recibido: 06/02/2020 / Aprobado: 17/07/2020 / Publicado en www.actagastro.org el 28/09/2020

Summary
Hepatic involvement due to syphilis is a rare manifestation where a high index of suspicion is required for its diagnosis. Three clinical cases of syphilitic hepatitis with cholestatic/mixed presentation are described and discussed, without criteria of severity and rapid biochemical response once the specific treatment has been administered.
Key words. Syphilis, hepatitis, cholestasic pattern.
Hepatitis sifilítica: ¿deberíamos agregarla al algoritmo de las alteraciones del hepatograma? Reporte de una serie de casos
Resumen
La afectación hepática de la sífilis es una manifestación poco común que requiere de un alto grado de sospecha para su diagnóstico. Se describen y discuten tres casos clínicos de hepatitis sifilítica con la presentación colestásica o mixta, sin criterios de gravedad y con una rápida respuesta bioquímica una vez administrado el tratamiento específico.
Palabras claves. Sífilis, hepatitis, patrón colestásico.
Introduction
Syphilis is a sexually transmitted systemic infectious disease caused by Treponema Pallidum, with high prevalence in at-risk populations.1, 2 Men who have sex with men (MSM) and those infected with human immunodeficiency virus (HIV) are the main risk groups. The most frequent route of transmission is sexual, and less commonly, oral.3 The progression of the disease is divided into three successive stages: the primary stage, characterized by the presence of the inoculation chancre, the secondary stage, characterized by mucocutaneous lesions and adenomegalies, and the tertiary stage where cardiological, ophthalmic, and auditory manifestations, as well as the presence of syphilitic gums are evident. In the absence of clinical manifestations, its diagnosis becomes extremely challenging.1, 2
Hepatic involvement is described in 0.2-3%, with higher prevalence in the secondary and tertiary stages as a result of the hematogenous dissemination of Treponema. In 90% of the cases there is an association with maculopapular rash in the torso and extremities and, in a smaller percentage, with genital symptoms (balanitis).3-9 The cholestatic pattern is the usual form of presentation, although mixed and necrotic forms have been reported.10 Positive results of the non-treponemal (VDRL or RPR) and treponemal (FTA-ABS, ELISA) serological tests, associated with clinical and biochemical improvement with treatment, after exclusion of other more frequent etiologies, allows to confirm the diagnosis.3 Histology is not relevant and the most frequent findings are: periportal lymphocytic infiltrate, focal necrosis, non-caseifying granulomas and in a minority of cases, the presence of spirochetes.11, 12 Although resolution is usually the norm, cases of fulminant hepatic failure have been reported.13-14
The aim of presenting this series of cases is to communicate the hepatic manifestation of a disease known for several decades, which is considered infrequent, but is probably under-diagnosed.
Clinical cases
Case 1
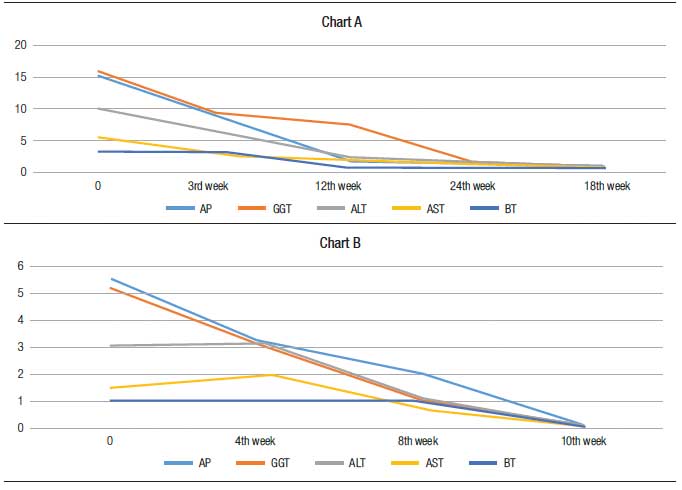
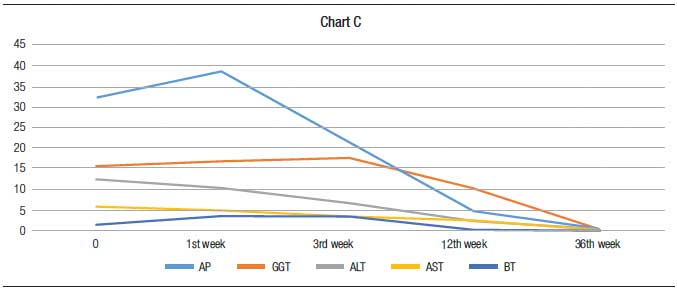
A 43-year-old man, without risk factors for liver disease, who consulted for pruritus and choluria of a week of evolution. He had no abdominal pain or fever. Jaundice was found on physical examination, without other alterations. The biochemichal tests on admission showed: total bilirubin (BT) 2.4 mg/dl, direct bilirubin (BD) 2.1 mg/dl, alkaline phosphatase (AP) 3270 U/L (240), GGT 512 U/L (33), AST 186 U/L (27), ALT 395 U/L (33), Total protein test 6.9 g/dl, PT 82% (70-100), hemoglobin 13.4 g/dl, platelets 326,000/mm3, white blood cells 7.7 103/uL (69% neutrophils, 15% lymphocytes, 3% eosinophils). Abdominal ultrasound and magnetic cholangioresonance (CRMN) excluded biliopancreatic pathology. Serology for hepatotropic viruses (IgM HAV, HBsAg, AntiHbc, AntiHBs, HCV ELISA), nonhepatotropics (CMV IgM, EBV IgM) and the autoimmunity panel (ANA, AMA, ASMA) were non-reactive. The electrophoretic proteinogram was normal and the HIV serology negative. Reactive TPHA and VDRL 1/64. Treatment with benzathine penicillin was initiated intramuscularly at a dose of 2,400,000 IU/per week, with a total of 3 doses. The patient showed clinical improvement after treatment was established. At 24 weeks of the start of treatment, hepatogram normalization and serological negativization were observed (Chart 1A).
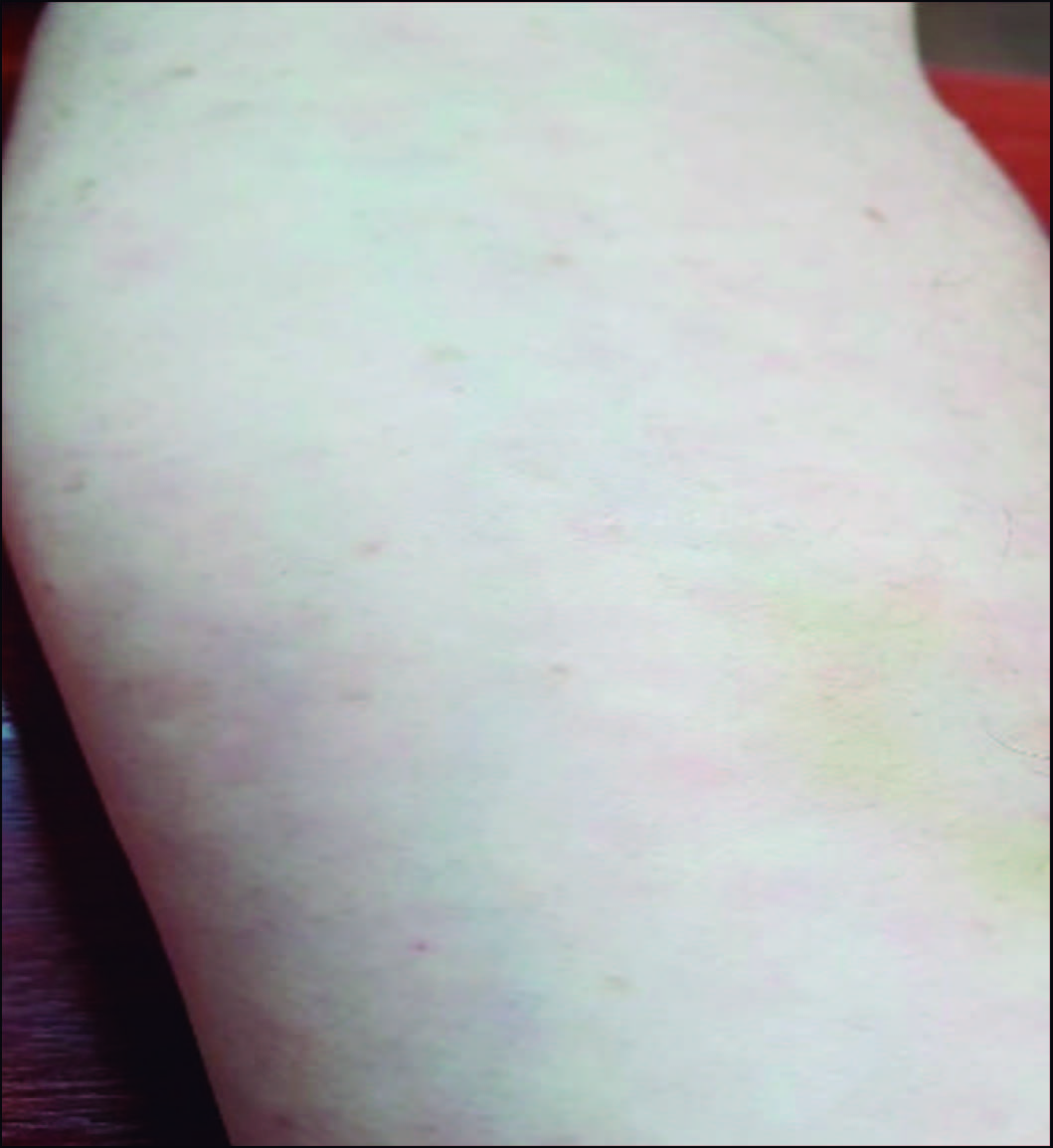
Chart 1. Biochemical evolution of clinical cases 1 (A), 2 (B), 3 (C). The values of AP, GGT, ALT and AST are represented in number of times over the normal value
Case 2
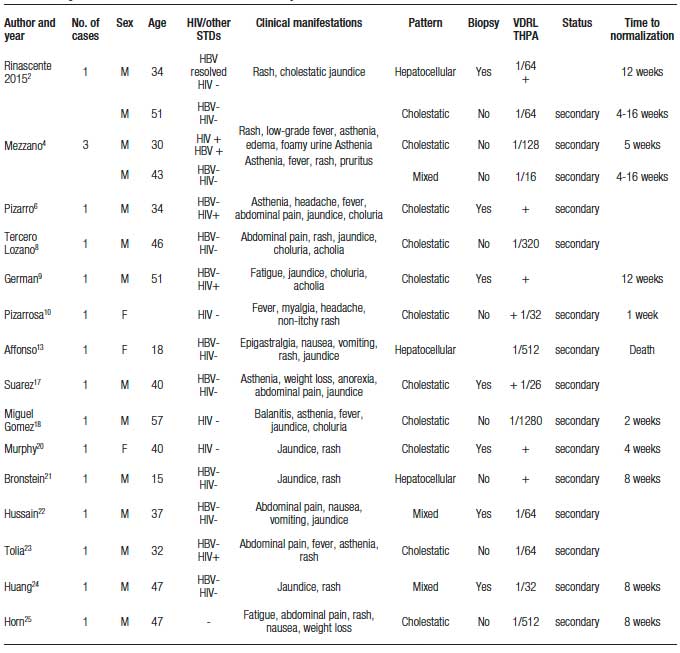
A 52-year-old man with a diagnosis of dyslipidemia and arterial hypertension, in treatment with atorvastatin and enalapril for 4 years. He consulted for pruritus, asthenia and adynamia of 2 weeks of evolution, without abdominal pain or fever. The examination showed hyperpigmented and pruritic macule lesions on the back of the arm and forearm (Figure 1).
Paraclinical tests showed: BT 2.8 mg/dl, BD 1.9 mg/dl, AP 646 U/L (240), GGT 219 U/L (33), AST 69 U/L (27), ALT 127 U/L (33), Total protein test 7.2 g/dl, PT 91% (70-100), hemoglobin 11.9 g/dl, platelets 458,000/mm3, white blood cells 6.8 103/uL (70% neutrophils, 12% lymphocytes, 2.8% eosinophils). Ultrasound and computed abdominal tomography (CAT) with contrast excluded biliopancreatic pathology. HIV, IgM HAV, HBsAg, IgM AntiHbc, HCV ELISA, CMV IgM and EBV IgM as well as autoimmunity (ANA, ASMA, AMA) were ruled out. Electrophoretic proteinogram was normal. Positivity of the VDRL (1/256) and TPHA allowed for a diagnosis of syphilitic hepatitis. Treatment with intramuscular 2,400,000 IU Benzatinic Penicillin was initiated, with clinical improvement and normalization of liver enzymes at 8 weeks (Chart 1B).
Figure 1. Macular exanthema in forearm (case report 2)
Case 3
A 39-year-old man with risky sexual behaviors and laparoscopic cholecystectomy for vesicular polyps in 2008. Routine examinations showed hepatogram abnormality. He was asymptomatic and the physical examination was normal. Paraclinical tests showed: BT 0.8 mg/dl, AP 725 U/L (240), GGT 449 U/L (33), AST 188 U/L (27), ALT 291 U/L (33). The serology of IgM HAV, HBsAg, AntiHbc IgM, HCV ELISA, CMV IgM and EBV IgM was negative. The HIV test was reactive and confirmed by viral load. Abdominal ultrasound showed no abnormalities. At 3 weeks the hepatogram showed: AP 3038 U/L (240), GGT 2194 U/L (33), AST 160 U/L (27), ALT 338 U/L (33). The serology for syphilis (VDRL 1/256 and TPHA) was positive and the treatment with Benzathine Penicillin 2,400,000 IU (3 doses) was initiated. 24 weeks after the initiation of the treatment, improvement of the hepatogram and the negativity of the serology were observed (Chart 1C).
Discussion
Syphilis is a sexually transmitted multisystemic disease that, despite being preventable and curable, constitutes a major health problem.5 It is known as “the great simulator” due to its various forms of presentation, in which pruritus, dermatological and genital manifestations are the most frequent.7 Hepatic involvement is rare and is generally considered in patients with risky sexual behavior after excluding other more frequent etiologies. The literature on syphilitic hepatitis is scarce and in the form of reports and case series.1-4, 6-25 There is only one systematic review in which 73 articles published between 1951 and 2017 were included, with 144 cases of syphilitic hepatitis. The average age was 40.5 years, the predominant sex was male (90.3%), 54.4% of the patients were homosexual and 61.4% had HIV. Almost 90% (88.9%) was in the early stages of syphilis (primary or secondary). Rash was the most frequent symptom (77.9%), followed by fatigue, anorexia (56.7%) and jaundice (35.1%). The cholestatic pattern was the most predominant and in 38% of the cases a liver biopsy was performed. All patients received antibiotic treatment (89.5% penicillin) and showed a good response.26
Table 1 describes the main characteristics of those reports and case series found in the literature and not included in the systematic review.
Table 1. Reports and case series not included in the systematic review
In this series the average age was 44 years, all were men, with cholestatic/ mixed pattern and one of them had HIV. In HIV-infected patients the prevalence of syphilitic hepatitis is 0.2-10% of the cases and, in general, this infection is contemplated within the differential diagnoses of liver profile alterations in this subgroup.1, 15, 16
Liver biopsy in syphilitic hepatitis is nonspecific and the presence of spirochetes can be difficult to demonstrate. Even in cases where immunohistochemistry or Warthin Starry staining was performed, the bacteria was found in 19 of the 28 cases.26
Treponema pallidum still presents extreme susceptibility to penicillin, so much so that there are no reports of resistant syphilis.5 The current recommendation for the treatment of early syphilis (primary and secondary) is the administration of benzathine penicillin G 2.4 million IU, in 1 to 3 doses, with cure rates reported between 80-95% at 6 months follow-up and normalization of the hepatogram occurring on average between 4 and 16 weeks after starting treatment.4, 5 Other alternatives to standard treatment with less evidence are doxycycline, ceftriaxone, tetracycline and azithromycin.4, 5, 11 The three cases reported in this series were treated with Benzathine Penicillin G and a few weeks after initiation, a significant improvement of the hepatogram was observed, with normalization between 10 and 36 weeks. Table 2 describes the main characteristics of the 3 cases described in this series. The rapid improvement in the alteration of the liver profile once the first dose of the treatment was administered would allow a diagnostic approach and thus subordinate the liver biopsy to those cases in which this improvement does not happen or there are other diagnostic hypotheses.
Table 2. Comparison of the main characteristics of the 3 clinical cases

Conclusion
The increase in the incidence of syphilis, the morbidity and mortality associated with its chronicity, the simplicity of its diagnosis and the effectiveness of its treatment, are sufficient arguments to consider investigating it in patients with cholestatic/mixed hepatitis even in the absence of risk factors.
Declaration of interest. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Syphilis as a diagnosis of liver abnormalities in HIV. Scand J Infect Dis 2013; 45: 703-705.
- Rinascente C, Candela G, Cervero M, Lobato A, Carbonell A. Acute non cholestasic hepatitis as the first manifestation of secondary syphilis. Rev Gastroenterol Perú 2015; 35: 247-249.
- Rubio-Tapia A, Hujoel IA, Smyrk TC, Poterucha JJ. Emerging secondary syphilis presenting as syphilitic hepatitis. Hepatology 2017; 65: 2113-2115.
- Mezzano G, Rondón F, Cid A, Parra F, Soto A, Gómez F. Hepatitis sifilítica: reporte de una serie de casos. Rev Med Chile 2019; 147: 251-255.
- Ministerio de Salud del Uruguay. Recomendaciones de diagnóstico, tratamiento y vigilancia de las infecciones de transmisión sexual 2016: 1-92.
- Pizarro R, Quezada M, Moreno F. Hepatitis sifilítica en paciente infectado con el virus de inmunodeficiencia humana. Rev Chil Infect 2001; 18: 143-146.
- Aggarwal A, Sharma V, Vaiphei K, Duseja A, Chawla YK. An unusual cause of cholestatic hepatitis: syphilis. Dig Dis Sci 2013; 58: 3049-3051.
- Tercero-Lozano M, Del Castillo-Codes I, Galvez-Fernández RM, Colmenero-Lechuga MM, Baeyens-Cabrera E. Hepatitis Sifilítica: una entidad poco frecuente. RAPD ONLINE 2013: 36: 131-133.
- German MN, Matkowskyj KA, Hoffman RJ, Agarwal PD. A case of syphilitic hepatitis in an HIV-infected patient. Hum Pathol 2018; 79: 184-187.
- Pizzarossa AC, Rebella M. Hepatitis in patients with syphilis: an overlooked association. BMJ Case Rep 2019; 12: 1-3.
- Bork JT, Macharia T, Choi J, Gilliam BL, Buchwald UK. Syphilitic Hepatitis Treated With Doxycycline in an HIV-Infected Patient and review of the literature. Sex transm Dis 2014; 41: 507-510.
- Ibáñez M, Varela M, Rodríguez-Peláez M, Mancebo A, García-Mayor MA, Pereira R. Luetic hepatitis. An emerging entity. Gastroenterol Hepatol 2009; 32: 610-613.
- Affonso da Costa AB, Fornazari B, da Silva FPM, Frandoloso GA, Breda GL. Fulminant hepatitis in a patient with secondary syphilis. Int J STD AIDS. 2018; 29:1348-1350.
- Lo JO, Harrison RA, Hunter AJ. Syphilitic hepatitis resulting in fulminant hepatic failure requiring liver transplantation. J Infect 2007; 54: 115-117.
- Adachi E, Koibuchi T, Okame M, Sato H, Kikuchi T, Koga M. Liver dysfunction in patients with early syphilis: a retrospective study. J Infect Chemother 2013; 19: 180-182.
- Manavi K, Dhasmana D, Cramb R. Prevalence of hepatitis in early syphilis among an HIV cohort. Int J STD AIDS 2012; 23: 4-6.
- Suarez Iznaga R. Hepatitis Sifílitica. Revista Cubana de Medicina 2012; 51: 272-277.
- De Miguel Gómez A, Benedicto Sánchez JR. Hepatitis sifilítica: una patología “poco frecuente”. Medifam 2002; 12: 108-109.
- Ridruejo E, Mordoh A, Herrera F, Avagnina A, Mando OO. Severe Cholestatic Hepatitis as the First Symptom of Secondary Syphilis. Dig Dis Sci 2004; 49: 1401-1404.
- Murphy CJ, Bhatt A, Chen W, Malli A, McGorisk T, Kelly SG. Syphilitic hepatitis. Lancet Gastroenterol Hepatol 2017; 2: 920.
- Bronstein FN, Meyer B, Condat B, Loria A, Bronstein JA.. Secondary syphilitic hepatitis in a fifteen-year-old boy. Med Mal Infect 2019; 49: 625-627.
- Hussain N, Igbinedion SO, Diaz R, Alexander JS, Boktor M, Knowles K. Liver Cholestasis Secondary to Syphilis in an Immunocompetent Patient. Case Reports Hepatol 2018; 2018: 8645068.
- Tolia S, Kassem H, Capatina-Rata A. The Great Impostor: transaminitis masking the coinfection of Syphilis and Human Immunodeficiency Virus. Case Rep Med 2017: 24819.
- Huang J, Lin S, Wang M, Wan B, Zhu Y. Syphilitic hepatitis: a case report and review of the literature. BMC Gastroenterol 2019; 19: 191.
- Horn CL, Jalali S, Abbott J, Stein MT. A Surprising Diagnosis: Syphilitic gastritis and hepatitis. Am J Med 2018: 131: 1178-1781.
- Huang J, Lin S, Wan B, Zhu Y. A Systematic Literature Review of Syphilitic Hepatitis in Adults. J Clin Transl Hepatol 2018; 28: 306-309.
Correspondencia: Victoria Veloso
Avenida Italia 2870. Montevideo, Uruguay
Correo electrónico: victoriavelosogiribaldi@gmail.com
Acta Gastroenterol Latinoam 2020;50(3):335-340
