Néstor A Gómez,1, 2 Stanley M Jama,3 Jorge O Gutiérrez4
1 Hospital Clínica Kennedy. Guayaquil.
2 School of Medicine. Universidad de Guayaquil. Guayaquil.
3 Hospital León Becerra. Milagro.
4 School of Medicine. Universidad Espíritu Santo. Samborondón.
Ecuador.
Acta Gastroenterol Latinoam 2018;48(4):310-313
Recibido: 20/09/2017 / Aprobado: 23/03/2018 / Publicado en www.actagastro.org el 17/12/2018

Summary
Aim. Report a case of appendix mucocele. This pathology consists of the mucinous accumulation in the lumen of the appendix that leads to dilatation with an incidence that ranges from 0.07% to 0.63%. Clinical case. A 70-year-old male patient was admitted in our department for a colonoscopy. He referred an intermittent pain in the lower right quadrant. During colonoscopy, an intraluminal round lesion in the cecum was found. Surgical excision was planned because of its size. Laparotomy via a Mc Burney incision was made, in which was found an appendix tumor. Intra-operative cold biopsy reported mucinous cystoadenoma of the appendix. The appendix and tumor were completely removed and the patient had an unremarkable post-operative.
Key words. Mucinous cystoadenoma, colonoscopy, appendix mucocele.
Mucocele apendicular
Resumen
Objetivo. Reportar un caso de mucocele apendicular. Esta patología consiste en la acumulación de mucina en el lumen del apéndice que produce una dilatación con una prevalencia de 0,07% al 0,63%. Caso clínico. Paciente de sexo masculino de 70 años que concurre a realizarse una colonoscopía por dolor intermitente en el cuadrante inferior derecho. Durante la colonoscopía se encontró una lesión redondeada intraluminal. Debido al tamaño, se programó la extirpación quirúrgica. Se realizó una laparotomía a través de una incisión de McBurney, en la que se encontró un tumor apendicular. La biopsia por congelación intraoperatoria reportó un cistoadenoma mucinoso del apéndice. El apéndice y el tumor fueron completamente removidos y el paciente tuvo un posoperatorio favorable.
Palabras claves. Cistoadenoma mucinoso, colonoscopía, mucocele apendicular.
Appendix mucocele (AM) is a dilatation of the appendix secondary to mucinous accumulation in the lumen regardless of the etiology. This pathology was first described by Karl Freiherr von Rokitansky in 1842.1 It affects both sexes equally and has an incidence that ranges from 0.07 to 0.63%, commonly appearing in the 5th to 7th decade of life.2 It has been described the association of AM with other tumors, been the colorectal, ovarium, breast, and liver tumor the most common.3 In the majority of the cases, AM is asymptomatic. When symptoms appear, patients refer right lower quadrant pain.4 Due to the lack of symptoms, it is diagnosed in advanced stages and historically it has been incidentally diagnosed during surgical intervention, endoscopic procedures or imaging studies.5 We present a male patient with mucinous cystoadenoma diagnosed during a colonoscopy.
Clinical case
A 70-year-old men was admitted in the Gastroenterology Department for a colonoscopy exam. At interrogation, he complained of abdominal pain located at the right lower quadrant for the past couple of years. The pain was mild, intermittent, non-radiating, and without aggravating or relieving factors. His past surgical history included cholecystectomy, prostatectomy, and right inguinal herniorrhaphy.
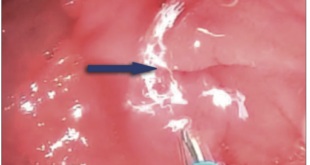
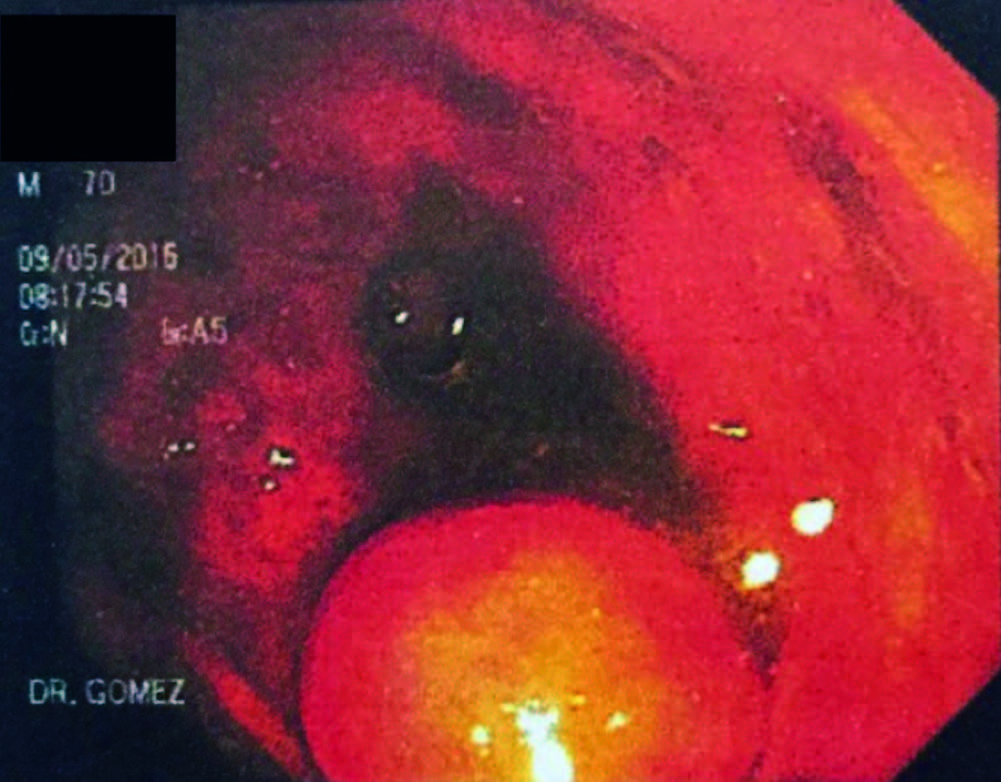
His physical examination was unremarkable. No abdominal tenderness, mass, or pain was found. During colonoscopy, an intraluminal round lesion, with a wide base located at the cecum in the appendix region, was found (Figure 1).
Figura 1. Colonoscopy view demonstrating an intraluminal rounded lesion located at the caecum.
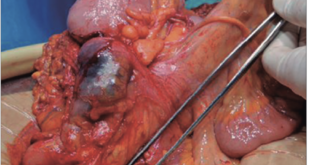
A tumor or polyp was suspected but, because of its size and the risk of leaving a posterior orifice that could complicate the patient`s prognosis, he was not colonoscopically intervened. Laboratory exams, including cell blood count and inflammatory markers where within normal parameters. The patient underwent a planned laparotomy via a McBurney incision. The findings revealed a nodular lesion of 1 to 1.5 cm implanted at the base of the appendix suggestive of an appendix tumor. The tumor and the appendix were removed through an appendectomy. Intra-operative cold biopsy was sent to the pathologist who reported an apparent mucinous cystoadenoma of the appendix. Abdominal cavity was closed and re-intervention was considered in case final histologic results changed. His postoperative course was uneventful. Histopathology reported a mucinous cystoadenoma macroscopically characterized by abundant mucinous material of white and transparent aspect with flattening of the mucosa and thinning of the walls (Figure 2).
Figura 2. (a) Excised distended appendix (b) Mucous content inside the appendix.


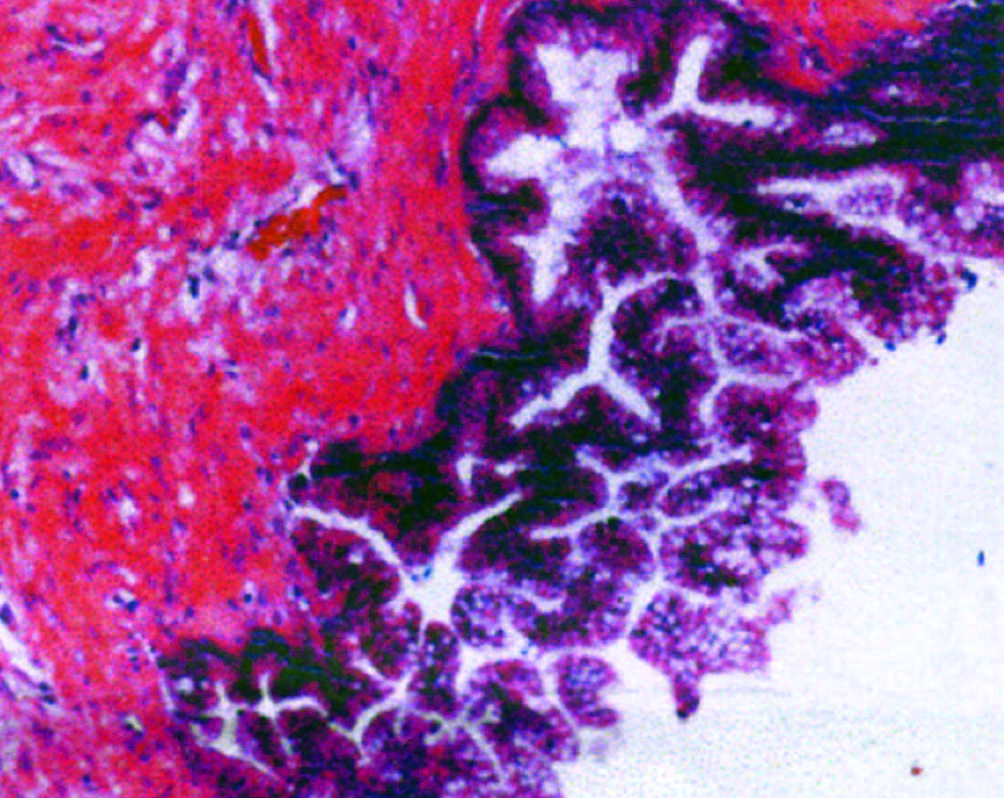
Microscopically, it presented proliferation of glandular structures of multiple shapes and forms with areas of flattening of the epithelium and atrophic aspect. No malignant activity was reported and the base of the appendix was free of neoplasia (Figure 3).
Figura 3. Microscopic examination demonstrating proliferation of glandular structures of different shapes along with atypical epithelial cells.
Discussion
Appendix mucocele can be caused by neoplasic and non-neoplasic hystologic lesions that includes: retention cyst, mucosal hyperplasia, mucinous cystoadenoma or mucinous cystoadenocarcinoma.6, 7 Mucinous cystoadenoma is the dilatation of the appendix with atypical and villous changes of the normal epithelium. Mucinous cystoadenoma is also referred as a low grade appendiceal mucinous neoplasm (LAMNs). LAMNs type 1 is when the lesion is confined inside the lumen, while in type 2 mucin is located outside the lumen.
Early diagnosis is important due to the possibility of malignancy or development of complications.8 The most feared complication of AM is pseudomixoma peritonei (PMP), the accumulation of mucinous neoplasic fluid in the peritoneal cavity that can lead to organ invasion. The most common cause of PMP is the perforation of the appendix. It presents as a progressive increase of the abdominal perimeter with symptoms related to organ invasion. Because of its widespread dissemination, management is a challenge.9 The best diagnostic tool for appendix mucocele is CT scan.10 It appears as a tubular or spheric well defined mass contiguous to the cecum of low attenuation material. Colonoscopy findings of AM include the “volcano sign”, an elevated lesion covered of normal mucosa with the appendiceal orifice located in the center or yellowish lipoma-like submucosal mass.5 Its treatment is based on the underlying cause and peritoneal invasion. An intra-operative frozen sectioning is important to determine the hystologic type and the type of surgery required. In patients with retention cyst, mucosal hyperplasia and LAMNs type 1 appendectomy is suggested.9 In case of benign lesions without positive margins of resection and perforation, appendectomy is recommended. If lymph nodes, positive margins of resection or cytology are present, right hemicolectomy and cytoreductive surgery (CRS) combined with heated intra-peritoneal chemotherapy (HIC) or early post-operative, intra-peritoneal chemotherapy (EPIC) should be considered.5
Conclusion
Appendix mucocele is the mucinous accumulation of the appendix lumen that produces dilatation caused by a variety of histologic types. Patients remain asymptomatic or refer vague symptoms leading it to an incidental diagnosis in imagenological studies. Because of its risk of perforation and producing pseudomyxoma peritonei, it is important the early recognition and surgically treatment of this disease. Intra-operative frozen sectioning is recommended in order to determine the histologic type and the appropriate surgical procedure.
Conflict of interest. This work complies with the requirements on informed consent / assent, ethics committee, funding, animal studies and on the absence of conflict of interests as appropriate.
References
- Jiménez Mazure C, Ramírez Plaza CP, Valle Carbajo M, Santoyo Santoyo J. Mucocele apendicular gigante. Implicaciones diagnósticas y terapéuticas. Rev Española Enfermedades Dig 2009; 101: 439-451.
- Rabie ME, Al Shraim M, Al Skaini MS, Alqahtani S, El Hakeem I, Al Qahtani AS et al. Mucus containing cystic lesions “mucocele” of the appendix: The unresolved issues. Int J Surg Oncol 2015; Article ID 139461, 9 pages.
- Utrillas Martínez AC, Muniesa Soriano JA, del Val Gil JM, Cruces Conde A, López Peris P, González Penabad M, et al. Mucocele Apendicular. Rev Española Enfermedades Dig 2008; 100: 730- 738.
- Echenique-Elizondo M, de Robles CL, Arratíbel Amondarain JA, Aribe X. Mucoceles apendiculares. Cir Esp 2007; 82: 297-300.
- Mastoraki A, Sakorafas G, Vassiliu P, Contopoulou C, Arkadopoulos N. Mucocele of the appendix: Dilemmas in differential diagnosis and therapeutic management. Indian J Surg Oncol 2016; 7: 86-90.
- Pilco P, Beltrán-flores S, López-Burga M. Cistoadenocarcinoma mucinoso de apéndice cecal. Rev Chil Cirugía 2016; 68: 319-322.
- Yoshida Y, Sato K, Tada T, Maekawa H, Sakurada M, Orita H et al. Two cases of mucinous cystadenoma of the appendix successfully treated by laparoscopy. Case Rep Gastroenterol 2013; 7: 44-48.
- Martinez-Gonzalez MD, Takahashi T, Robles-Atayde JA, Lome C, Gamboa-Domínguez A, Bezaury P et al. Mucocele del Apéndice Vermiforme. Rev Gastroenterol Mex 1996; 61: 366-370.
- Rymer B, Forsythe RO, Husada G. Mucocoele and mucinous tumours of the appendix: A review of the literature. Int J Surg 2015; 18: 132-135.
- Agrusa A, Romano G, Galia M, Cucinella G, Sorce V. Appendiceal mucinous neoplasms: an uncertain nosological entity. Report of a case. G di Chir 2016; 37: 86-89.
Correspondencia: Néstor A Gómez
Tel.: +593-997725769
Correo electrónico: ngomez@gye.satnet.net
Acta Gastroenterol Latinoam 2018;48(4): 310-313