Callie Cuff ID· Rena Yadlapati ID
University of California San Diego, Division of Gastroenterology.
San Diego, CA, USA.
Acta Gastroenterol Latinoam 2025;55(4):292-302
Received: 06/11/2025 / Accepted: 11/12/2025 / Published online: 23/12/2025 / https://doi.org/10.52787/agl.v55i4.555

Summary
The concept of laryngopharyngeal reflux has evolved since it was first used to describe the retrograde flow of gastric contents into the upper airway leading to upper airway symptoms. Decades of cross-disciplinary research have led to our current understanding of this process, which emphasizes differentiating laryngopharyngeal reflux disease (characterized by symptoms with objective evidence of reflux) from laryngopharyngeal symptoms (which can occur with or without pathological reflux). It is essential to recognize this distinction for effective management because laryngopharyngeal reflux disease may respond to anti-reflux therapy, whereas the management of laryngopharyngeal symptoms depends on the clinical entity or entities contributing to them. This review summarizes the historical development of the laryngopharyngeal reflux concept, outlines current diagnostic and therapeutic approaches for laryngopharyngeal reflux disease, and highlights ongoing challenges and opportunities for future research. We conclude that continued interdisciplinary collaboration is essential for improving both evidence-based diagnoses and effective treatment outcomes.
Keywords. Laryngopharyngeal reflux, Gastroesophageal reflux, Esophageal pH Monitoring, Laryngopharyngeal reflux disease, Diagnostic framework.
Reflujo laringofaríngeo: perspectivas históricas, diagnósticos y tratamientos actuales, y desafíos pendientes
Resumen
El concepto de reflujo laringofaríngeo ha evolucionado desde que se utilizó por primera vez para describir el flujo retrógrado del contenido gástrico hacia las vías respiratorias superiores provocando síntomas. Décadas de investigación interdisciplinaria condujeron a nuestra comprensión actual del proceso, que indica la importancia de diferenciar la enfermedad por reflujo laringofaríngeo (caracterizada por síntomas con evidencia objetiva de reflujo) de los síntomas laringofaríngeos (que pueden ocurrir con o sin reflujo patológico). Es esencial reconocer esta distinción para hacer un tratamiento eficaz, ya que la enfermedad por reflujo laringofaríngeo puede responder al tratamiento antirreflujo, mientras que el tratamiento de los síntomas laringofaríngeos depende de la entidad o entidades clínicas que contribuyen a que estos ocurran. En esta revisión se resume el desarrollo histórico del concepto de reflujo laringofaríngeo, se esbozan los enfoques diagnósticos y terapéuticos actuales de la enfermedad por reflujo laringofaríngeo y se destacan los retos actuales y las oportunidades para la investigación futura. Concluimos que la colaboración interdisciplinaria continua es esencial para mejorar tanto los diagnósticos basados en la evidencia como los resultados de los tratamientos.
Palabras claves. Reflujo laringofaríngeo, reflujo gastroesofágico, monitorización del pH esofágico, enfermedad por reflujo laringofaríngeo, marco de diagnósticos.
Abbreviations
LPRD: laryngopharyngeal reflux disease.
LPS: laryngopharyngeal symptpms.
GERD: gastroesophageal reflux disease.
PPI: proton pump inhibitor.
LRT: Laryngeal Recalibration Therapy.
Introduction
Traditionally, the term laryngopharyngeal reflux (LPR) has been used to describe the retrograde flow of gastric content into the larynx and pharynx, resulting in a spectrum of upper airway symptoms. Laryngopharyngeal symptoms (LPS) include chronic cough, throat clearing, hoarseness, and postnasal drip, which can occurr without classic symptoms of heartburn or regurgitation. Symptoms in this region can arise from various sources, including airway diseases, such as asthma or allergic rhinitis, or gastrointestinal disorders, such as gastroesophageal reflux disease (GERD) or esophageal motility disorders, with contributions from neurosensory or behavioral factors. Laryngopharyngeal reflux disease (LPRD) is defined as the presence of objective evidence linking reflux to LPS, which distinguishes it from symptoms without measurable reflux events. LPS account for up to 10% of otolaryngology and gastroenterology referrals and are commonly treated with empiric proton pump inhibitor (PPI) therapy.1, 2 However, objective testing suggests that fewer than half of patients with these symptoms have confirmed reflux-related pathology.3, 4 The high rate of misattributing LPS to LPRD highlights the importance of a thorough evaluation to avoid misdiagnosis, unnecessary interventions, and prolonged symptom burden. Distinguishing between reflux-mediated symptoms and those arising from non-gastrointestinal etiologies is essential for guiding appropriate evaluation and treatment. However, the diversity of potential contributors has made accurate diagnosis and effective management challenging since LPR was first described. This review summarizes our current knowledge of LPRD, outlining its historical background, current diagnostic and therapeutic approaches, and highlighting the remaining gaps in clinical understanding and management. In conclusion, we emphasize the need for a unified, evidence-based framework that integrates reflux physiology, laryngeal sensory function, and interdisciplinary collaboration to improve diagnosis and treatment outcomes.
History of laryngopharyngeal reflux
In 1968, Cherry described the association between reflux and laryngeal injury with the identification of laryngeal contact ulcers and granulomas as a manifestation of acid exposure5 (Figure 1).
Figure 1. Timeline of key milestones in the understanding of laryngopharyngeal reflux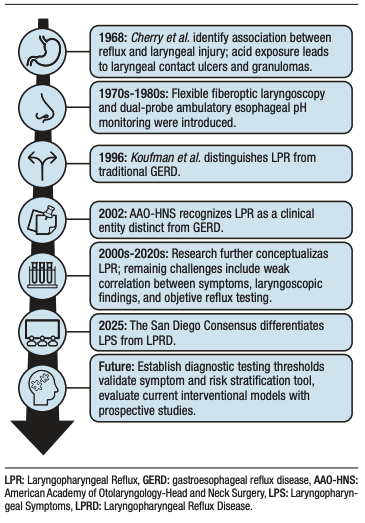
Following the introduction of flexible fiberoptic laryngoscopy and dual-probe ambulatory esophageal pH monitoring in the 1970s and 1980s, Koufman and colleagues characterized the clinical syndrome of LPR in 1996, highlighting its distinction from classic GERD.6 A few years later, in 2002, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) formally defined LPR as a clinical entity distinct from GERD, noting that LPR often presents without typical heartburn or regurgitation.7 In 2005, Ford published a widely cited review summarizing the evaluation and management of LPR. This review helped to establish standardized clinical approaches and guided subsequent research.8 It characterized the typical constellation of LPS and laryngoscopic findings attributed to reflux, emphasized empiric high-dose PPI therapy as both a diagnostic and therapeutic tool, and provided an early framework for distinguishing LPR from classic GERD. Over the subsequent decades, several groups sought to further refine LPR, but gaps in our understanding persisted. These gaps included poor correlation between symptoms, laryngoscopic findings, and objective reflux testing, as well as the lack of a gold standard for diagnosis. These limitations led to the 2025 San Diego Consensus, an international interdisciplinary initiative that aimed to further develop the nosology by differentiating LPS, which may or may not arise from LPRD, defined by laryngopharyngeal symptoms with objective evidence of reflux. The San Diego Consensus offered diagnostic criteria and recommended objective testing modalities in addition to summarizing the pathophysiology of these syndromes. This review described the Consensus’ recommendations.9
Pathophysiology and Mechanisms
LPRD arises through both direct chemical injury and complex neurosensory mechanisms. When refluxate containing acid, pepsin, and bile salts repeatedly contacts the laryngeal mucosa, it can disrupt epithelial tight junctions, impair barrier function, and trigger local inflammatory cascades, including cytokine and chemokine release. This leads to edema, erythema, and chronic laryngeal inflammation.10, 11 Pepsin remains stable at neutral pH and can be reactivated by intermittent acid exposure, causing subclinical epithelial injury even when overt reflux is minimal. Bile salts further exacerbate mucosal damage through oxidative stress and mitochondrial dysfunction, promoting epithelial apoptosis and tissue remodeling.10, 11 This inflammatory environment sensitizes laryngeal sensory nerves, lowering the threshold for coughing, throat clearing, globus sensation, and other laryngopharyngeal symptoms. Chronic peripheral stimulation also primes central neural circuits, amplifying symptom perception through central sensitization.10, 11
Beyond gastroesophageal and neurosensory mechanisms, several airway and non-gastrointestinal factors can mimic or exacerbate LPS. Chronic postnasal drip from allergic rhinitis or sinusitis, asthma-related cough reflex sensitization, and environmental irritants can trigger laryngeal inflammation or hypersensitivity.12, 13 Similarly, vocal overuse or muscle tension dysphonia may sustain symptoms independent of reflux physiology.14
Even when the underlying cause of reflux is addressed, LPS may persist with anti-reflux therapy, reflecting the contribution of neurogenic or behavioral factors in patients with LPRD. Vagal-mediated reflexes, heightened laryngeal sensory responses, and central sensitization can cause the larynx to become hypersensitive or hyperresponsive, leading to chronic symptoms, even when there is no acid exposure.4, 7-10
Mechanistic studies suggest that abnormal vagal signaling and impaired baroreflex sensitivity amplify sensory input, increasing awareness of normal laryngeal sensations and promoting maladaptive throat behaviors.8, 9 Persistent activation of laryngeal sensory pathways may sensitize central circuits, resulting in chronic, self-perpetuating symptoms.8 Behavioral interventions such as laryngeal recalibration therapy provide evidence that targeted sensory retraining can reduce symptom burden, supporting the role of neurogenic and behavioral mechanisms.7, 10 Similar to what has been observed in disorders of gut–brain interaction (DGBIs), emerging evidence suggests that the microbiome may influence the development or persistence of LPS. Specifically, some research suggests that altered laryngopharyngeal microbial communities and acid suppression–induced dysbiosis may contribute to local inflammation and vagal signaling, further promoting laryngeal hypersensitivity.11-13
Together, these findings support a multifactorial model in which LPRD involves direct mucosal injury and neurogenic dysfunction. Similarly, the persistence of LPS despite investigation and treatment of non-gastrointestinal or airway causes may be due to laryngeal hypersensitivity and behavioral factors described above.
Clinical Presentation
Patients with LPRD may experience various aerodigestive symptoms, including chronic cough, persistent throat pain or irritation, frequent throat clearing, excess phlegm or postnasal drip sensations, and hoarseness. A globus sensation is another common complaint, though it is less frequently related to underlying reflux physiology than thepreviously described symptoms.9 Patients may initially present with these symptoms to primary care clinicians or various specialists, such as gastroenterologists, otolaryngologists, or pulmonologists, depending on their predominant symptoms. When patients present with these complaints, providers should screen for additional red flag signs that may indicate malignancy or other serious pathology, such as hemoptysis, progressive dysphagia, odynophagia, unexplained weight loss, or a neck mass. These signs warrant urgent evaluation.15
Outside of urgent presentations, there is significant variation in diagnostic approaches among practitioners, likely due to the absence of a gold standard for diagnosis.16 Many patients may undergo multiple procedures and numerous specialist visits, which lead to a substantial economic and time burden.10, 17 One study found that the mean direct cost over the first year of evaluation for suspected extraesophageal reflux is 5.6 times higher than those reported for typical GERD.18 Over half of these expenditures are driven by prescription medications, particularly proton pump inhibitors, which may or may not be warranted as first-line therapy. Beyond the financial and time burden, patients’ quality of life may be further impacted by heightened symptom perception, symptom-related anxiety, and substantial psychosocial distress.19
Diagnostic Evaluation
The evaluation of LPS typically follows a stepwise approach. It begins with a symptom assessment and progresses to an endoscopic evaluation, reflux testing, or empiric therapy, based on the clinical presentation and suspicion of reflux-related disease (Figure 2). The San Diego Consensus emphasized that symptoms must occur at least twice weekly and be present for over eight weeks to qualify as LPS, and highlights the need to consider non-gastrointestinal causes. Various instruments have been developed to characterize the multifaceted presentation of LPS. Patient-reported outcomes (PROs) measurements and risk stratification tools can be helpful for initial evaluations, these lack sufficient specificity to establish a definitive diagnosis. For example, the Reflux Symptom Index (RSI) is a patient-reported measure of symptom severity; however, it lacks specificity for LPRD and is used in other reflux conditions.20 The COuGH RefluX and HAs-BEER (Heartburn, Asthma, and BMI Extraesophageal Reflux) Scores serve as risk stratification tools and offer complementary information about reflux-related susceptibility.21, 22 The Laryngeal Cognitive Assessment Tool (LCAT) explores cognitive and brain–gut contributions to symptom experience. While it is not diagnostic for LPRD, it can inform a more holistic understanding of the patient perception.23 After taking a thorough clinical history, directly visualizing the larynx is a useful next step in the evaluation process if non-gastrointestinal etiologies are suspected.
Figure 2. Diagnostic and therapeutic schema for evaluating laryngopharyngeal symptoms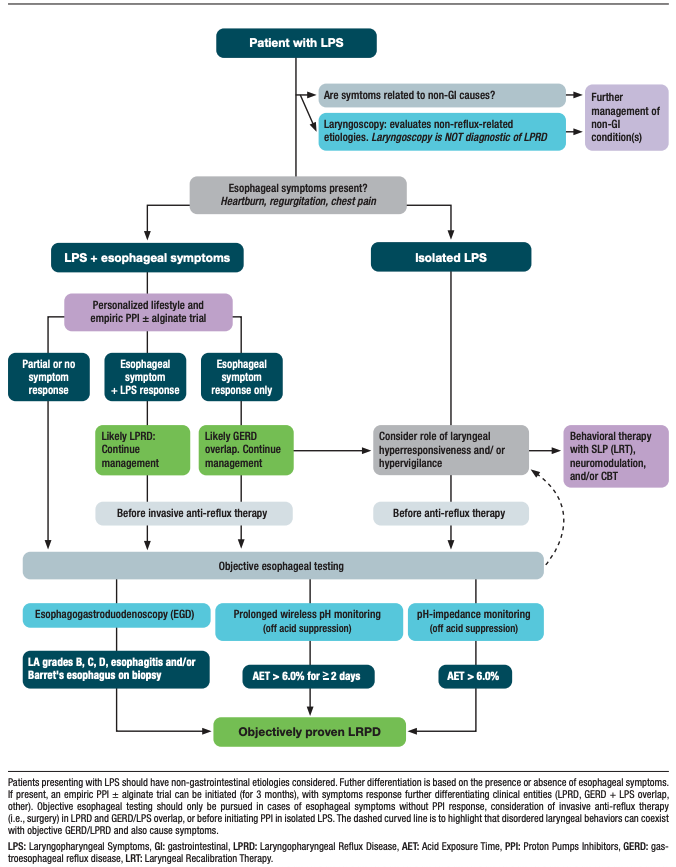
The primary role of laryngoscopy is to evaluate non-reflux-mediated processes that contribute to LPS, such as structural lesions or vocal fold pathology. “Classic” inflammatory findings, such as posterior laryngeal erythema, edema, or pseudosulcus are nonspecific and cannot confirm LPRD by themselves.9 In patients with isolated LPS (without esophageal symptoms) that are not attributable to non-gastrointestinal causes or that persist despite appropriate treatment, the focus of further evaluation should be on laryngeal hyperresponsiveness and hypervigilance before anti-reflux treatment, as well as on objective esophageal testing to evaluate for LPRD/GERD.
If esophageal symptoms such as heartburn, regurgitation, or chest pain are also present, high-dose empiric PPI therapy can be started to evaluate the patient’s response to treatment. Dosing is typically twice daily for up to three months and this remains a common first-line strategy. Patients who improve in both esophageal symptoms and LPS following PPI initiation, likely have LPRD. An isolated esophageal symptom response to PPI therapy suggests LPS and GERD overlap. For patients with partial or no symptom response to PPI, objective reflux testing is strongly recommended. This testing is also recommended for patients with a positive symptom response to PPI therapy before therapy is escalated or invasive interventions are considered. Testing should be performed while the patient is off acid-suppressing therapy.
Direct visualization of the esophagus via esophagogastroduodenoscopy (EGD) can be used to investigate evidence of GERD, with findings of Los Angeles grades B, C, D esophagitis and/or biopsy-proven Barrett’s esophagus as confirmatory.24 Inlet patches of ectopic gastric mucosa in the esophagus may also be present and contribute to globus or irritation through their secretion of acid, mucus, or pepsin, though further investigation is needed, however, to establish whether ablation significantly reduces LPS burden.25 Transnasal esophagoscopy offers a minimally invasive, in-office assessment of the proximal esophagus, but should be reserved for providers with specialized training.9 If endoscopic findings of reflux are absent, reflux monitoring can be pursued to further investigate its presence.
Available modalities include 96-hour extended wireless pH monitoring, 24-hour combined impedance-pH, hypopharyngeal and esophageal multichannel intraluminal impedance-pH (HEMII-pH).26 – 28 Wireless pH and pH-impedance are currently the primary instruments to diagnose reflux in LPRD. Both measure acid exposure time (AET) in the distal esophagus. An AET > 6.0% on either study (and over two or more days on the 96-hour study) is confirmatory of GERD/LPRD.24, 28, 29 While prolonged wireless pH monitoring improves day-to-day reproducibility compared with single-day impedance testing, it lacks impedance-based detection of nonacid reflux. However, there are currently no validated standalone thresholds for nonacid reflux and interobserver variability in interpreting impedance data and laryngoscopic findings complicates cross-study comparisons. HEMII-pH provides superior characterization of mixed and weakly acidic events, both proximally and distally, but it remains technically complex and less widely available.27 There is no universal acceptance of the thresholds used to define abnormal proximal acid reflux, which limits the standardization of HEMII-pH across practices.30 Beyond these modalities, salivary pepsin assays have shown potential as a noninvasive adjunctive test, but they have not yet been validated for routine diagnosis.31 In contrast, standalone oropharyngeal pH monitoring has demonstrated poor reproducibility and limited correlation with objectively confirmed reflux events, so it is not recommended for the diagnosis of LPRD.32, 33
Management Strategies
Management of LPRD and LPS is multimodal and tailored to symptom severity, objective evidence of reflux, and the presence of laryngeal hypersensitivity (Table 1). Initial management should focus on behavioral and lifestyle modifications, escalation to pharmacologic therapy and, when appropriate, procedural interventions for patients with persistent or objectively confirmed reflux.
Table 1. Summary of Management Strategies for laryngopharyngeal reflux disease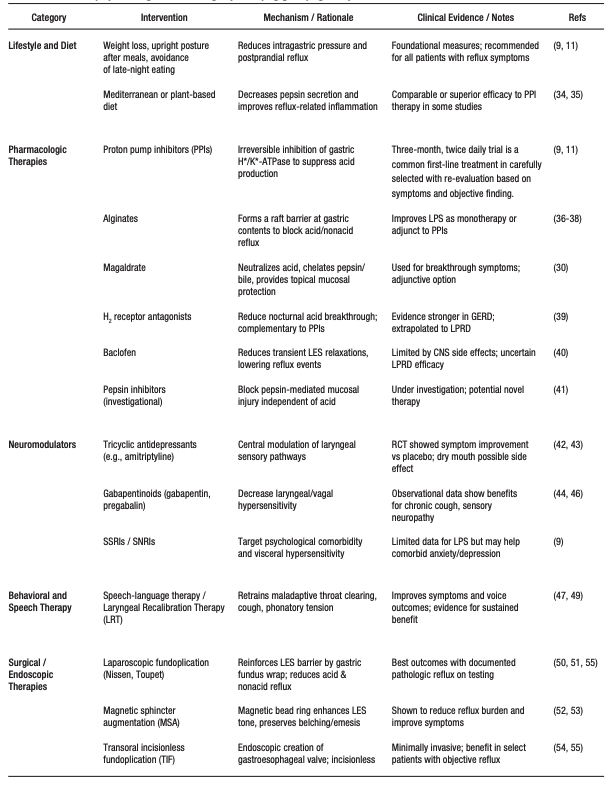
Lifestyle and dietary measures are first-line treatments for patients with combined laryngopharyngeal and esophageal symptoms. These include losing weight to reduce intragastric pressure, avoiding late-night meals and maintaining an upright position for two to three hours after eating to minimize post-prandial reflux, and/or modifying sleeping positions to reduce nocturnal reflux. Dietary approaches include adopting a plant-forward or Mediterranean-style diet, which is thought to work by decreasing pepsin secretion. These strategies have shown benefit comparable to or exceeding those of pharmacologic therapy in some studies.34, 35
Pharmacologic treatment often begins with a three-month, twice daily PPI trial, as previously described, but alternative or adjunctive agents also exist. Alginates form a viscous gel “raft” that physically blocks reflux and reduces laryngeal exposure to gastric contents.36 Their use four times daily (after meals and before bed) has shown to decrease LPS alone37 or as an adjunct to PPI therapy.38 Magaldrate is a topical antacid that neutralizes acid and chelates pepsin and bile. It can also be used as an adjunct for breakthrough symptoms.30 H2 receptor antagonists can provide additional acid suppression, particularly for nocturnal reflux. They may complement PPI therapy, though this has been more studied in GERD.39 If these are ineffective, baclofen may be considered to reduce transient lower esophageal sphincter relaxations, thereby decreasing reflux episodes. However, its use may be limited by central nervous system side effects and it’s benefit for extraesophageal reflux is uncertain.40 Finally, pepsin inhibitor, such as fosamprenavir, which target the proteolytic activity of pepsin, may prevent mucosal injury independent of acid suppression, though their use is still investigational.41
For patients whose symptoms reflect or are compounded by laryngeal hypersensitivity rather than direct reflux injury, neuromodulators such as low-dose tricyclic antidepressants (TCAs), gabapentin, or pregabalin, can help reduce neurogenic cough or throat sensations.9 A randomized controlled trial by Jang et al. demonstrated that amitriptyline significantly improved chronic laryngopharyngeal neuropathy symptoms compared with placebo,42 though the anticholinergic effects of TCAs may also lead to dry mouth and worsen LPS.43 Observational studies support the use of gabapentinoids for refractory sensory neuropathies involving the larynx44, 45 and for chronic cough symptoms resulting from vagal-mediated hypersensitivity.46 In patients with LPS and coexisting anxiety or depression, other neuromodulatory medications such as selective serotonin reuptake inhibitors or serotonin–norepinephrine reuptake inhibitors may provide symptomatic benefit. This pattern is also seen in disorders of gut-brain interaction (DGBI), although data specific to LPS are limited.9
Behavioral approaches, including speech-language–guided laryngeal therapy or laryngeal recalibration therapy (LRT), aim to retrain maladaptive behaviors such as throat clearing, chronic coughing, and hyperresponsive vocal fold.47, 48 These interventions combine breathing retraining, phonatory control, and desensitization techniques to normalize sensory perception and reduce inappropriate laryngeal muscle activation. In a recent prospective study, LRT significantly improved symptom burden and perceptual voice outcomes in patients with suspected LPRD.47 Evidence from related voice and cough disorders supports the use of speech-language therapy as a first-line or adjunctive strategy for laryngeal hypersensitivity, providing long-term benefits when combined with reflux management or neuromodulator therapy.16, 47 49
Surgical or endoscopic interventions, such as laparoscopic fundoplication, magnetic sphincter augmentation (MSA), or transoral incisionless fundoplication (TIF), are generally reserved for carefully selected patients with objectively documented pathologic reflux who continue to experience symptoms despite optimized medical and behavioral therapy.9
Laparoscopic fundoplication, which is most commonly performed using a Nissen or Toupet technique, strenghens the lower esophageal sphincter (LES) by wrapping the gastric fundus around the distal esophagus, thereby reducing both acid and nonacid reflux events.50, 51 Magnetic sphincter augmentation employs a ring of magnetic beads placed around the LES to increase sphincter tone while preserving physiologic ability to belch and vomit.52, 53 Transoral incisionless fundoplication is an endoscopic alternative that reconstructs the gastroesophageal valve through a transoral approach. This avoids abdominal incisions and offers a less invasive option for select patients.54
While surgical interventions can improve reflux burden and reduce laryngeal symptoms in patients with confirmed extraesophageal reflux, outcomes are highly dependent on appropriate patient selection. Meta-analyses indicate that surgical success is greatest when abnormal esophageal acid exposure or impedance events are documented preoperatively. Patients with isolated laryngeal symptoms and normal reflux testing derive less benefit.55, 56 Consequently, current consensus guidelines emphasize that anti-reflux surgery should be pursued only after objective evidence of reflux is confirmed and non-reflux mechanisms of laryngopharyngeal symptoms have been excluded.9, 55
Finally, integration of multidisciplinary care is increasingly recognized as crucial for managing LPS and LPRD. Gastroenterologists, otolaryngologists, speech-language pathologists, dieticians, and behavioral health specialists can collaborate to address the interplay of reflux, hypersensitivity, and psychosocial factors, tailoring therapy to individual patients.
Future Directions
Future efforts in LPRD are focused on refining diagnostic precision and advancing patient-centered care. Ongoing interdisciplinary research aims to establish clear, evidence-based thresholds for pH-impedance and proximal esophageal acid exposure, as well as validate symptom and risk stratification tools that can reliably distinguish reflux-related disease from other laryngeal disorders. It is equally important to develop and validate robust patient-reported outcome measures and conduct long-term prospective studies to evaluate the comparative effectiveness of medical, behavioral, and surgical interventions. Longitudinal phenotyping could eventually allow tailored therapy based on reflux burden, sensory phenotype, and psychosocial profile. A personalized, multidisciplinary model that integrates gastroenterology, otolaryngology, speech-language pathology, and behavioral health is increasingly recognized as essential to address the complex interplay of reflux, laryngeal hypersensitivity, and neurogenic factors in individual patients. Together, these efforts will help tailor therapy, avoid overtreatment, and optimize long-lasting symptom relief for diverse patient populations.
Conclusion
Since its initial description, the concept of LPR has been clouded by symptom overlap with other gastrointestinal and airway disorders. Careful evaluation of patients with LPS should include exclusion of non-reflux etiologies and, when appropriate, objective reflux testing to confirm LPRD. For patients with confirmed LPRD, treatment plans should emphasize evidence-based strategies for controlling reflux and multidisciplinary support for managing laryngeal hypersensitivity. Continued interdisciplinary collaboration between gastroenterology, otolaryngology, speech-language pathology, and behavioral health is essential for advancing both diagnostic precision and therapeutic outcomes. To achieve these goals, future research should aim to establish diagnostic thresholds, validate or develop new symptom and risk stratification tools, and refine treatment pathways.
Intellectual property. The authors declare that the data and figures presented in the manuscript are original and were carried out at their belonging institutions.
Funding. The author declares that there were no external sources of funding.
Conflict of interest. The author declares that he has no conflicts of interest in relation to this article.
Copyright

© 2025 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Cuff C and Yadlapati R. Laryngopharyngeal Reflux: Historical Perspectives, Current Diagnostics and Therapies, and Remaining Challenges. Acta Gastroenterol Latinoam. 2025;55(4):292-302. https://doi.org/10.52787/agl.v55i4.555
References
- Lechien JR, Saussez S, Schindler A, Karkos PD, Hamdan AL, Harmegnies B, et al. Clinical outcomes of laryngopharyngeal reflux treatment: A systematic review and meta-analysis. Laryngoscope. 2019;129(5):1174-87.
- Yadlapati R, Katzka DA. Laryngopharyngeal Reflux Is an Eternally Rolling Boulder. Clin Gastroenterol Hepatol. 2020;18(7):1431-2.
- Krause AJ, Carlson DA, Chan WW, Chen CL, Gyawali CP, Laryngeal Symptoms Working G, et al. High Diagnostic Yield of Abnormal Endoscopic Findings in the Evaluation of Laryngopharyngeal Reflux. Clin Gastroenterol Hepatol. 2024;22(8):1741-3 e1.
- Lee YC, Lee JS, Kim SW, Kwon KH, Eun YG. Influence of age on treatment with proton pump inhibitors in patients with laryngopharyngeal reflux disease: a prospective multicenter study. JAMA Otolaryngol Head Neck Surg. 2013;139(12):1291-5.
- Cherry J, Margulies SI. Contact ulcer of the larynx. Laryngoscope. 1968;78(11):1937-40.
- Koufman J, Sataloff RT, Toohill R. Laryngopharyngeal reflux: consensus conference report. J Voice. 1996;10(3):215-6.
- Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg. 2002;127(1):32-5.
- Ford CN. Evaluation and management of laryngopharyngeal reflux. JAMA. 2005;294(12):1534-40.
- Yadlapati R, Weissbrod P, Walsh E, Carroll TL, Chan WW, Gartner-Schmidt J, et al. The San Diego Consensus for Laryngopharyngeal Symptoms and Laryngopharyngeal Reflux Disease. Am J Gastroenterol. 2025.
- Blaine-Sauer S, Bock J, Bor S, Allen J, Randall DR, Mittal S, et al. Extraesophageal reflux: Clinical manifestations and tools for diagnosis and treatment. Ann N Y Acad Sci. 2025;1547(1):233-44.
- Cui N, Dai T, Liu Y, Wang YY, Lin JY, Zheng QF, et al. Laryngopharyngeal reflux disease: Updated examination of mechanisms, pathophysiology, treatment, and association with gastroesophageal reflux disease. World J Gastroenterol. 2024;30
(16):2209-19. - Canning BJ, Chang AB, Bolser DC, Smith JA, Mazzone SB, McGarvey L, et al. Anatomy and neurophysiology of cough: CHEST Guideline and Expert Panel report. Chest. 2014;146
(6):1633-48. - Bucca CB, Bugiani M, Culla B, Guida G, Heffler E, Mietta S,
et al. Chronic cough and irritable larynx. J Allergy Clin Immunol. 2011;127(2):412-9. - Franco RA, Andrus JG. Common diagnoses and treatments in professional voice users. Otolaryngol Clin North Am. 2007;
40(5):1025-61, vii. - Lechien JR, Saussez S, Muls V, Barillari MR, Chiesa-Estomba CM, Hans S, et al. Laryngopharyngeal Reflux: A State-of-the-Art Algorithm Management for Primary Care Physicians. J Clin Med. 2020;9(11).
- Krause AJ, Walsh EH, Weissbrod PA, Taft TH, Yadlapati R. An update on current treatment strategies for laryngopharyngeal reflux symptoms. Ann N Y Acad Sci. 2022;1510(1):5-17.
- Gyawali CP, Carlson DA, Chen JW, Patel A, Wong RJ, Yadlapati RH. ACG Clinical Guidelines: Clinical Use of Esophageal Physiologic Testing. Am J Gastroenterol. 2020;115(9):1412-28.
- Francis DO, Rymer JA, Slaughter JC, Choksi Y, Jiramongkolchai P, Ogbeide E, et al. High economic burden of caring for patients with suspected extraesophageal reflux. Am J Gastroenterol. 2013;108(6):905-11.
- Liu K, Krause AJ, Greytak M, Taft T, Walsh E, Yadlapati R. Psychosocial burden in patients with chronic laryngopharyngeal symptoms with and without pathologic acid reflux. Neurogastroenterol Motil. 2024;36(9):e14852.
- Abraham ZS, Kahinga AA. Utility of reflux finding score and reflux symptom index in diagnosis of laryngopharyngeal reflux disease. Laryngoscope Investig Otolaryngol. 2022;7(3):785-9.
- Krause AJ, Kaizer AM, Carlson DA, Chan WW, Chen CL, Gyawali CP, et al. Validated Clinical Score to Predict Gastroesophageal Reflux in Patients With Chronic Laryngeal Symptoms: COuGH RefluX. Clin Gastroenterol Hepatol. 2024;22(6):1200-9 e1.
- Patel DA, Sharda R, Choksi YA, Slaughter JC, Higginbotham T, Garrett CG, et al. Model to Select On-Therapy vs Off-Therapy Tests for Patients With Refractory Esophageal or Extraesophageal Symptoms. Gastroenterology. 2018;155(6)
1729-40 e1. - Krause AJ, Yadlapati R, Wong MW, Taft T, Pandolfino JE, Gyawali CP, et al. Validation of the Laryngeal Cognitive-affective Tool in a Taiwanese Population. J Clin Gastroenterol. 2024.
- Gyawali CP, Yadlapati R, Fass R, Katzka D, Pandolfino J, Savarino E, et al. Updates to the modern diagnosis of GERD: Lyon consensus 2.0. Gut. 2024;73(2):361-71.
- Dunn JM, Sui G, Anggiansah A, Wong T. Radiofrequency ablation of symptomatic cervical inlet patch using a through-the-scope device: a pilot study. Gastrointest Endosc. 2016;84(6):
1022-6 e2. - Lechien JR. Clinical Update Findings about pH-Impedance Monitoring Features in Laryngopharyngeal Reflux Patients. J Clin Med. 2022;11(11).
- Lechien JR, Bobin F. Variability and accuracy of multiple saliva pepsin measurements in laryngopharyngeal reflux patients. J Otolaryngol Head Neck Surg. 2023;52(1):66.
- Yadlapati R, Masihi M, Gyawali CP, Carlson DA, Kahrilas PJ, Nix BD, et al. Ambulatory Reflux Monitoring Guides Proton Pump Inhibitor Discontinuation in Patients With Gastroesophageal Reflux Symptoms: A Clinical Trial. Gastroenterology. 2021;160(1):174-82 e1.
- Yadlapati R, Gyawali CP, Masihi M, Carlson DA, Kahrilas PJ, Nix BD, et al. Optimal Wireless Reflux Monitoring Metrics to Predict Discontinuation of Proton Pump Inhibitor Therapy. Am J Gastroenterol. 2022;117(10):1573-82.
- Lechien JR. Pharmacological and Biological Relevance in the Medical Treatment of Laryngopharyngeal Reflux: A State-of-the-Art Review. J Voice. 2024.
- Jing W, Luo W, Lou L. Diagnostic utility of salivary pepsin in laryngopharyngeal reflux: a systematic review and meta-analysis. Braz J Otorhinolaryngol. 2023;89(2):339-47.
- Desjardin M, Roman S, des Varannes SB, Gourcerol G, Coffin B, Ropert A, et al. Pharyngeal pH alone is not reliable for the detection of pharyngeal reflux events: A study with oesophageal and pharyngeal pH-impedance monitoring. United European Gastroenterol J. 2013;1(6):438-44.
- Yadlapati R, Adkins C, Jaiyeola DM, Lidder AK, Gawron AJ, Tan BK, et al. Abilities of Oropharyngeal pH Tests and Salivary Pepsin Analysis to Discriminate Between Asymptomatic Volunteers and Subjects With Symptoms of Laryngeal Irritation. Clin Gastroenterol Hepatol. 2016;14(4):535-42 e2.
- Snow G, Dhar SI, Akst LM. How to Understand and Treat Laryngopharyngeal Reflux. Gastroenterol Clin North Am. 2021;50(4):871-84.
- Zalvan CH, Hu S, Greenberg B, Geliebter J. A Comparison of Alkaline Water and Mediterranean Diet vs Proton Pump Inhibition for Treatment of Laryngopharyngeal Reflux. JAMA Otolaryngol Head Neck Surg. 2017;143(10):1023-9.
- Leiman DA, Riff BP, Morgan S, Metz DC, Falk GW, French B, et al. Alginate therapy is effective treatment for gastroesophageal reflux disease symptoms: a systematic review and meta-analysis. Dis Esophagus. 2017;30(2):1-8.
- McGlashan JA, Johnstone LM, Sykes J, Strugala V, Dettmar PW. The value of a liquid alginate suspension (Gaviscon Advance) in the management of laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2009;266(2):243-51.
- Reimer C, Lodrup AB, Smith G, Wilkinson J, Bytzer P. Randomised clinical trial: alginate (Gaviscon Advance) vs. placebo as add-on therapy in reflux patients with inadequate response to a once daily proton pump inhibitor. Aliment Pharmacol Ther. 2016;43(8):899-909.
- Mainie I, Tutuian R, Castell DO. Addition of a H2 receptor antagonist to PPI improves acid control and decreases nocturnal acid breakthrough. J Clin Gastroenterol. 2008;42(6):676-9.
- Vaezi MF, Katzka D, Zerbib F. Extraesophageal Symptoms and Diseases Attributed to GERD: Where is the Pendulum Swinging Now? Clin Gastroenterol Hepatol. 2018;16(7):1018-29.
- Johnston N, Samuels TL, Goetz CJ, Arnold LA, Smith BC, Seabloom D, et al. Oral and Inhaled Fosamprenavir Reverses Pepsin-Induced Damage in a Laryngopharyngeal Reflux Mouse Model. Laryngoscope. 2023;133 Suppl 1(Suppl 1):S1-S11.
- Jang M, Rubin SJ, Stein DJ, Noordzij JP. Randomized double blind trial of amitriptyline versus placebo in treatment of chronic laryngopharyngeal neuropathy. Am J Otolaryngol. 2017;38(6):683-7.
- Jeyakumar A, Brickman TM, Haben M. Effectiveness of amitriptyline versus cough suppressants in the treatment of chronic cough resulting from postviral vagal neuropathy. Laryngoscope. 2006;116(12):2108-12.
- Miller N, Noller M, Yang A, McCoul ED, Tolisano AM, Riley CA. Lesser Known Uses of gamma-Aminobutyric Acid Analogue Medications in Otolaryngology. Laryngoscope. 2022;132
(5):954-64. - Halum SL, Sycamore DL, McRae BR. A new treatment option for laryngeal sensory neuropathy. Laryngoscope. 2009;119
(9):1844-7. - Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet. 2012;380(9853):1583-9.
- Walsh E, Krause AJ, Greytak M, Kaizer AM, Weissbrod PA, Liu K, et al. Laryngeal Recalibration Therapy Improves Laryngopharyngeal Symptoms in Patients With Suspected Laryngopharyngeal Reflux Disease. Am J Gastroenterol. 2024;119
(11):2198-205. - Algara MA, Chan WW. Update on laryngopharyngeal reflux disease. Curr Opin Gastroenterol. 2025;41(4):251-9.
- Park JO, Shim MR, Hwang YS, Cho KJ, Joo YH, Cho JH, et al. Combination of voice therapy and antireflux therapy rapidly recovers voice-related symptoms in laryngopharyngeal reflux patients. Otolaryngol Head Neck Surg. 2012;146(1):92-7.
- Lee R, Mittal RK, Chang KJ, Nguyen NT. Nature of antireflux barrier formed by Nissen fundoplication surgery. Sci Rep. 2025;15(1):34047.
- Bredenoord AJ, Draaisma WA, Weusten BL, Gooszen HG, Smout AJ. Mechanisms of acid, weakly acidic and gas reflux after anti-reflux surgery. Gut. 2008;57(2):161-6.
- Maret-Ouda J, Markar SR, Lagergren J. Gastroesophageal Reflux Disease: A Review. JAMA. 2020;324(24):2536-47.
- Sterris JA, Dunn CP, Bildzukewicz NA, Lipham JC. Magnetic sphincter augmentation versus fundoplication for gastroesophageal reflux disease: pros and cons. Curr Opin Gastroenterol. 2020;36(4):323-8.
- Bazerbachi F, Krishnan K, Abu Dayyeh BK. Endoscopic GERD therapy: a primer for the transoral incisionless fundoplication procedure. Gastrointest Endosc. 2019;90(3):370-83.
- Chen JW, Vela MF, Peterson KA, Carlson DA. AGA Clinical Practice Update on the Diagnosis and Management of Extraesophageal Gastroesophageal Reflux Disease: Expert Review. Clin Gastroenterol Hepatol. 2023;21(6):1414-21 e3.
- Lechien JR, Dapri G, Dequanter D, Rodriguez Ruiz A, Marechal MT, De Marrez LG, et al. Surgical Treatment for Laryngopharyngeal Reflux Disease: A Systematic Review. JAMA Otolaryngol Head Neck Surg. 2019;145(7):655-66.
Correspondence: Callie Cuff
Email: ccuff@health.ucsd.edu
Acta Gastroenterol Latinoam 2025;55(4):292-302

