Beatriz Iade,1 Gaby Beatriz Buenavida,2 Andrea Casañas3
1 Gastroenterology Clinic, Hospital de Clínicas – Faculty of Medicine UDELAR.
2 Centro de Asistencia del Sindicato Médico del Uruguay (CASMU).
3 Sociedad Médica Quirúrgica de Salto/Centro de Asistencia Médica (CAM).
Acta Gastroenterol Latinoam 2018;48(4):263-270
Recibido: 27/09/2017 / Aprobado: 02/07/2018 / Publicado en www.actagastro.org el 17/12/2018

Summary
Incidence of inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC), seems to be increasing, but data about IBD epidemiology in Latin America remains scarce. This study aimed to determine the incidence of IBD in Uruguay for the period 2007-2011. A retrospective, registry-based study was performed, with data between January 2007 and December 2011 of two medical centers from Uruguay – Montevideo (220,687 members) and Salto (51,235 members). Patients were excluded if the diagnosis occurred outside this period, if it was not confirmed after one year of follow-up or if presenting unclassified IBD. Poisson regression was used to evaluate differences in incidence rates by sex and age at diagnosis. The U Mann Whitney test and Fisher’s exact test were used to compare age at diagnosis and sex distribution between centers and UC vs. CD patients. 67 new IBD cases were identified during 2007-2011. The adjusted IBD incidence was 5.22 /105 person-years with a UC/CD ratio of 7.7. Overall, women presented higher incidence of IBD (3.54 /105 person-years, p-value = 0.028). Incidence was also higher for patients aged 20-44 years (9.12 /105 person-years). Among IBD patients, 65.7% were female, mean age at diagnosis was 37.2 ± 17.25 years and 10.4% had family history of IBD. There were no significant differences between centers regarding sex and age at diagnosis of IBD patients. Despite industrialization, Uruguay continues to be a region of low IBD incidence, with UC being more common than CD. This trend is in line with epidemiological data from other Latin American countries.
Key words. Inflammatory bowel disease, ulcerative colitis, Crohn’s disease, incidence.
Incidencia de la enfermedad inflamatoria intestinal en dos centros médicos en Uruguay durante el período 2007-2011
Resumen
La incidencia de la enfermedad inflamatoria intestinal (EII), incluyendo la enfermedad de Crohn (EC) y la colitis ulcerosa (CU), sigue aumentando, pero los datos epidemiológicos de América Latina son escasos. Se realizó un estudio retrospectivo (registro de enero de 2007 a diciembre de 2011 de dos centros médicos de Uruguay) para determinar la incidencia de EII en Uruguay entre 2007 y 2011. Los pacientes fueron excluidos si el diag nóstico se produjo fuera de este período; si no, se confirmó después de un año de seguimiento o si presentaban EII no clasificada. Una regresión de Poisson para evaluar las diferencias en las tasas de incidencia por sexo y edad, al momento del diagnóstico, ha revelado que las mujeres presentaron mayor incidencia de EII (3,54/105 años-persona, p = 0,028). La incidencia también fue mayor para los pacientes de 20-44 años de edad (9,12/105 años-persona). Se utilizaron pruebas de Mann Whitney y exacta de Fisher para comparar la edad al diagnóstico y la distribución de sexos entre los centros. No hubo diferencias significativas entre los centros. Se identificaron 67 nuevos casos de EII. La incidencia ajustada de EII fue de 5,22/105 años-persona con una proporción CU/EC de 7,7. Entre los pacientes con EII, el 65,7% eran mujeres, la edad promedio al momento del diagnóstico fue de 37,2 ± 17,25 años y el 10,4% tenía antecedentes familiares de EII. Uruguay sigue siendo una región de baja incidencia de EII, y la CU es más frecuente que la EC, en concordancia con los datos latinoamericanos.
Palabras claves. Enfermedad inflamatoria intestinal, colitis ulcerosa, enfermedad de Crohn, incidencia.
Abbreviations
IBD: inflammatory bowel diseases.
CD: Crohn’s disease.
UC: ulcerative colitis.
RNEII: the National IBD Registry.
UDELAR: la Universidad de la República – Uruguay.
CASMU: Centro de Asistencia del Sindicato Médico del Uruguay.
Inflammatory bowel diseases (IBD) comprise mainly Crohn’s disease (CD) and ulcerative colitis (UC), for which treatment remains challenging.1, 2 With episodes of relapse and remission, it is one of the most severe gastrointestinal disorders, with relevant health and economic burden.3-5
IBD are characterized by chronic inflammation of the digestive mucosa, resulting from the interaction between genetic and environmental factors that triggers an excessive mucosal immune response.6-8 A number of environmental risk factors have been explored, including smoking, diet, breastfeeding, antibiotics, but the association of some of these factors with IBD is still inconsistent.6 Epidemiological studies may provide relevant information about IBD, its risk factors and clinical management.7, 9
Globally, the prevalence of IBD is estimated to be around 396 per 105 people.10 The incidence of inflammatory bowel disease (IBD) has been increasing in several world regions, namely in developing countries.9 Since its first description, IBD was more relevant in developed countries from North America and Europe, but the incidence and prevalence of CD and UC are now increasing in other geographical areas with previous low incidence, such as South and Eastern Europe and Asia.9-13 This trend in reported incidence and prevalence rates may be explained partially by the advances in disease diagnosis, but continued environmental changes may also impact IBD onset.4
Data about IBD epidemiology in Latin America is scarce and mostly based on hospital and retrospective records.14-17 A study conducted by Linares et al. reported incidences of 2.2 per 105 inhabitants in Argentina and 1.2 per 105 in Panama, during 1987-1993 period.18 Other recent studies in Brazil, Puerto Rico and Colombia have shown an increasing trend, similar to the evolution in high incidence areas.16, 17, 19-21
The National IBD Registry (RNEII, for its Spanish acronym) was created in 2006 and in 2008 it was declared of public interest by the Ministry of Health. This order applies to all medical institutions in Uruguay, whether public or private, enabling the collection of data from endoscopy files, pathology, pharmacy and clinical records that are required to identify new cases.22
Based on this registry, a (crude) incidence rate of 2.63 per 105 inhabitants/year was observed for the period 2007-2008,22 a lower rate in comparison with Puerto Rico, Colombia and Brazil.14, 18
This study aimed to determine the incidence of IBD (CD and UC) in two areas of Uruguay (Salto and Montevideo) for the period 2007-2011, and to compare the results with previous ones from Uruguay and those from other geographical regions.
Methods
A retrospective, registry-based study was performed, with data collection between January 1st 2007 and December 31st 2011 at two medical centers from Montevideo and Salto. Written informed consent was given by all study participants prior to inclusion. The study protocol was approved by the Ethics Committee of the Faculty of Medicine – UDELAR (La Universidad de la República – Uruguay).
Population
Uruguay is a country in South America with 176,215 km2 and a total population of 3.3 million people, of whom 1.8 million live in the metropolitan area of its capital and largest city, Montevideo. Salto region is one department of Uruguay and Salto is the third largest city of Uruguay, with 124.878 inhabitants.23 The majority of Uruguayans have Spanish and Italian origins, followed by French, German and other European origins; 87.4% of the population are Caucasian, 9.1% are Afro-descendants and 2.9% are aborigines. Male/female ratio is 0.93.24
Two medical centers were selected among those with complete information. The Montevideo center (CASMU – Centro de Asistencia del Sindicato Médico del Uruguay) is a private medical center with an average of 220,687 members. In Salto, IBD cases were identified among 51.365 patients followed up in a private medical center (CAM – Sociedad Médica Quirúrgica de Salto/ Centro de Asistencia Médica), during the study period. Both centers cover approximately 8% of the population in Uruguay.
Inclusion and exclusion criteria
The study included both outpatients and inpatients, with a new case of IBD (UC or CD) diagnosed between January 1st, 2007 and December 31st 2011, that received surgery or not and irrespective of treatment status. Patients were excluded from the study if the disease had started before or after this date, if the diagnosis was not confirmed after one year or if the colitis was unclassified.
The active search included not only endoscopy, pathology registries and medical records, but also administrative and pharmacy databases. When a potential case was identified, a medical appointment was scheduled with the patient to obtain the patient’s informed consent and fill in a RNEII form that includes data about IBD type, gender, age and place of residence at onset. The case was confirmed according to standard protocol after review by the principal investigators and a one year of follow up.
Statistical methods
The IBD incidence rates and specific incidence rates for UC and CD were calculated as the number of new cases for 100,000 patients-year. Demographic data of the year 2007, retrieved from the Uruguay National Institute of Statistics was assumed for the standardization of incidence rates.25 Differences in incidence rates by sex and age at diagnosis (0–19; 20–44; 45 years or older) were evaluated using Poisson regression models. The U Mann Whitney test was used to compare age at diagnosis between CASMU-Montevideo vs. CAM-Salto and UC vs. CD patients. Fisher’s exact test was used to compare sex distribution between CASMU-Montevideo vs. CAM-Salto and UC vs. CD patients.
Data were analyzed using the Statistical Package for the Social Sciences (version 21.0, SPSS, Chicago, IL) and the statistical package R (version 3.1.2, 2014). Significance level was set at 0.05.
This study was conducted within the RNEII framework. The RNEII was approved by the School of Medicine’s Ethics Committee and its public interest was recognized by the Uruguay Health Ministry in 2008.
Results
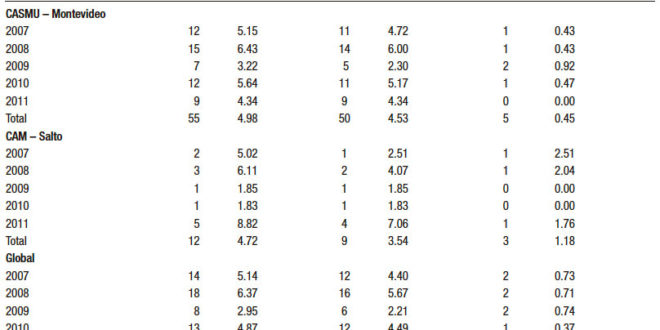
In the two centers, a total of 67 new IBD cases were identified during the period between 2007 and 2011. The crude incidence rate of IBD during the period 2007- 2011 was 4.94 per 105 person-years, 4.35 for UC and 0.59 for CD. After adjustment, the IBD incidence was 5.22 per 105 person-years, 4.62 for UC and 0.60 for CD, with a UC/ CD ratio of 7.7. For each center, the crude incidence rates of IBD were 4.98 per 105 person-years in CASMU-Montevideo, and 4.72 per 105 person-years in CAM-Salto (Table 1). Regarding, the incidence rates of IBD according to sex (Table 2), the crude incidence rates were 3.54 and 6.22 per 105 person-years, and the adjusted incidence rates were 3.80 and 6.59 per 105 person-years, for male and female sex, respectively. Overall, women presented significantly higher incidence rate of IBD (p = 0.028).
The incidence rates of IBD for patients aged ≤19 years (3.45 per 105 person-years) and for patients aged ≥ _45 years (2.92 per 105 person-years) were significantly lower (p = 0.005 and p < 0.001, respectively) than for patients aged 20- 44 years (9.12 per 105 person-years).
In CASMU-Montevideo, the crude incidence rate by age group was 4.04 per 105 person-years (< 19 years), 9.15 per 105 person-years (for 20-44 years), and 2.89 per 105 person-years (> 45 years). In CAM-Salto, the crude incidence rate by age group was 1.50 (< 19 years), 9.00 (for 20-44 years), and 3.04 (> 45 years) per 105 person-years (Table 2).
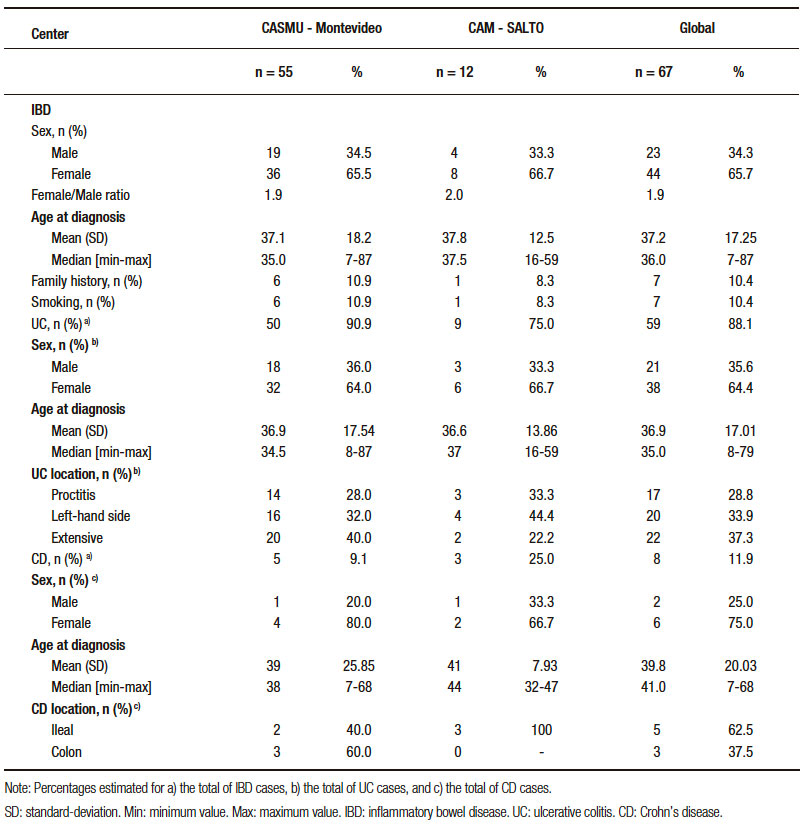
Table 3 presents the main characteristics of the IBD patients. No significant differences were found between UC and CD patients regarding sex (p = 0.711) and age at diagnosis (p = 0.568). The location in the UC was proctitis in 17 patients, left-sided in 20, and extensive in 22 of which 3 required surgery (colectomy). The location on the CD was ileal in 5, colon in 3; there were 0 cases with perineal involvement and 1 required surgery during the study period.
There were no statistically significant differences between centers regarding sex (p = 0.705) and age at diagnosis (p = 0.641) of IBD patients. In CASMU-Montevideo, the location in the UC was proctitis in 14 patients, left-hand side in 16, and extensive in 20 of which 3 required surgery (colectomy). Regarding CD, there were no cases with perineal involvement and none required surgery during the study period.
In CAM-Salto, the location in the UC was proctitis in 3 patients, left-hand side in 4, and extensive in 2; no patient required surgery. There were no CD cases with perineal involvement. One CD patient required surgery during the study period.
Table 1. Incidence rate of IBD in Montevideo and Salto, 2007-2011.

Table 2. Incidence rates of IBD by age and sex, 2007-2011
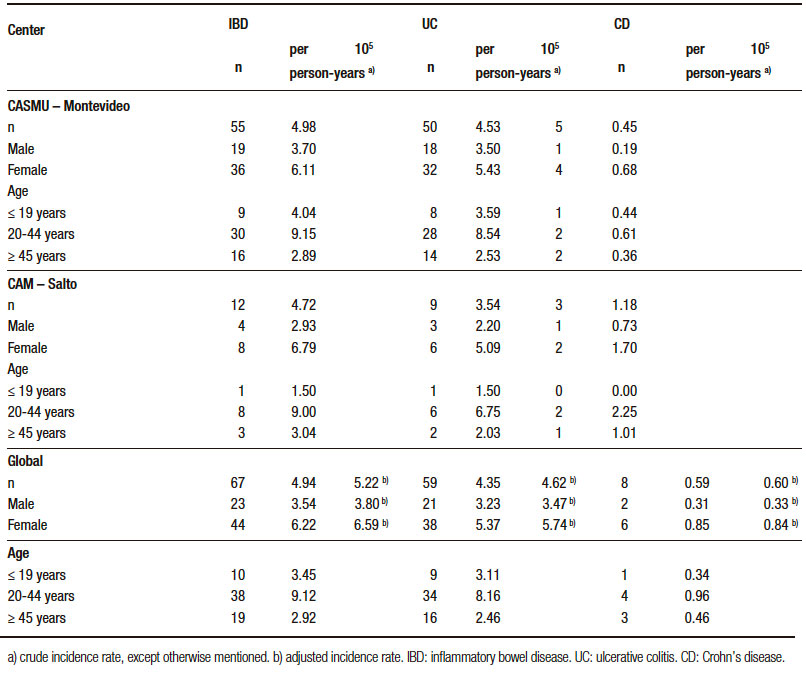
Table 3. Characteristics of IBD patients in Montevideo and Salto, 2007-2011.
Discussion
The observed IBD incidence was in accordance with a previous RNEII study and confirms Uruguay as one region of low IBD incidence.22 UC was more common than CD, as it has been described in other low incidence countries, including Brazil, Puerto Rico, Colombia, and Chile-14, 19, 26-28 In fact, the highest frequency of UC vs. CD is in line with the worldwide epidemiological data which shows that the increase of IBD follows a pattern where the increase of the UC precedes 15 to 20 years the increase of CD.10, 26
In North America and Europe, there has been an increase of IBD incidence, being estimated that the annual incidence of CD is higher in North America (20.2 /105 person-years), whereas the annual incidence of UC is higher in Europe (24.3 /105 person-years).4, 29 In our study, we have observed cumulative adjusted incidence of 5.22 /105 person-years. This lower IBD incidences are in line with the results from other Latin American countries, that reported incidences of UC ranging from 0.7 up to 6.8 per 105 people, between 1986 and 2008.26
In Brazil16, 21 and Mexico,30 the incidence of UC has been increasing. Furthermore, CD seems also to be increasing in Brazil.16, 21 The situation in Brazil is different from 1993 data from Argentina18 and from a previous study in Uruguay,22 where the reported incidence of IBD has been lower. Buenavida et al. have reported an adjusted incidence rate of 4.01 per 105 people for IBD during the biennial 2007 and 2008, considering 5 geographical areas in Uruguay.22 The higher incidence observed in 2011 in Salto could be related with the few cases identified in the whole period. The incidence in Montevideo did not show remarkable differences during this period.
Similar to what was reported by Buenavida et al., IBD was more frequent among women than among men.10, 22
The same trend was observed in data from Colombia,14 Brazil16, 27 and Chile28 and for UC patients in Puerto Rico.19
Age at diagnosis were similar between centers and somewhat lower than what was reported by Buenavida et al. (40.7 years), but within the range reported in other Latin American countries.22 For instance, a single center study in Brazil has reported a mean age at diagnosis of 35.2 years, while in Colombia the mean age was 40 years.14, 31 The two centres provided age data grouped into different classes. For this reason, data was reclassified to enable comparisons, which could have partially explained why the group of highest incidences were aged between 20 and 44 years. Nevertheless, Yepes Barreto et al. also observed that 49.9% of IBD patients were aged 20-44 years.14 Of notice, this study included pediatric patients (aged ≥ 7years) and the decrease in age at diagnosis seems to be aligned with the increase incidence of pediatric IBD worldwide.32
It is not expected that the low IBD incidence may have resulted from a detection bias, since the included centers were well equipped for the diagnosis and multiple data sources were used. The small number of cases, especially in Salto, may have affected the accuracy of the results, although the sample characteristics are similar to those described by others.22 The included centers are representative of the two regions, and no selection bias is expected since 94% of the population in Uruguay has access to health care. Furthermore, adjusted and crude incidence rates were similar, underlining that population from these two centers had a similar age and sex distribution.33
With growing industrialization, it is likely that, over the next years, there will be an increase of IBD in some areas of Central and South America, including Uruguay.26 In fact, IBD seems to occur most often in urban areas than in rural areas. The industrialization and urbanization of societies are associated with changes in microbial exposure, sanitation, occupations, diet, lifestyle, medications, and exposure to pollution, which have been implicated as possible risk factors environmental IBD.6 Additional follow-up of IBD epidemiology is required in Uruguay, to follow-up the impact of industrialization. This study provides insight about the evolution of IBD epidemiology in two main regions in Uruguay, with results confirming this country as a low incidence region. In the future, the analysis of data from RNEII could provide more evidence about the time trends of IBD and etiology of IBD, supporting the development of health care resources.
Acknowledgements. The authors wish to thank to Alejandro Noria (Quantitative Methods Department – Faculty of Medicine UDELAR) for the statistical analysis and assistance, Sergio Dotta (responsible for medical archive) at CASMU and to the staff from medical archive at CAM, Gustavo Burroso et al. (pharmacy services – CASMU), Cecilia Vazquez, Sabrina Villarroya, Adrian Canavesi, Marlene Faust for the data collection at CASMU, the collaboration of José Pedro Ibargoyen and Prof. Carlos Ketzoian (research coordinator at Hospital de Clínicas). The authors wish to thank for the acknowledgement of the medical writing assistance Milene Fernandes (Eurotrials, Scientific Consultants) and the financial support of AbbVie Inc. (Argentina).
Financial support. AbbVie Inc. (Argentina) supported medical writing services through Eurotrials, Scientific Consultants. AbbVie was not involved in the development of content of the manuscript and the authors maintained a complete control over the content. The authors had no other additional financial support.
Institutional review board statement. The study protocol was approved by the Institutional Review Board (Ethics Committee of the Faculty of Medicine UDELAR, Exp. Nº 071140-000236-06).
Informed consent statement. Written informed consent was given by all participants of the study prior to inclusion. The study protocol was approved by the Institutional Review Board (Ethics Committee of the Faculty of Medicine UDELAR, Exp. Nº 071140-000236-06).
Biostatistics statement. The statistical methods of this study were reviewed by Alejandro Noria, from the Quantitative Methods Department – Faculty of Medicine UDELAR, Montevideo, Uruguay. Statistical methods in this study are adequate and appropriate for the objectives and results studies.
Conflict-of-Interest statement. BI has received speaker fees from AbbVie and project grants from AbbVie and Janssen. The remaining authors have no conflicts of interest to report.
References
- Karlinger K, Gyorke T, Mako E, Mester A, Tarjan Z. The epidemiology and the pathogenesis of inflammatory bowel disease. European Journal of Radiology 2000; 35: 154-167.
- Moreau J, Mas E. Drug resistance in inflammatory bowel diseases. Current Opinion in Pharmacology 2015; 25: 56-61.
- Button LA, Roberts SE, Goldacre MJ, Akbari A, Rodgers SE, Williams JG. Hospitalized prevalence and 5-year mortality for IBD: record linkage study. World Journal of Gastroenterology 2010; 16: 431-438.
- Ponder A, Long MD. A clinical review of recent findings in the epidemiology of inflammatory bowel disease. Clinical Epidemiology 2013; 5: 237-247.
- Burisch J, Jess T, Martinato M, Lakatos PL. The burden of inflammatory bowel disease in Europe. Journal of Crohn’s & Colitis 2013; 7: 322-337.
- Molodecky NA, Kaplan GG. Environmental risk factors for inflammatory bowel disease. Gastroenterol Hepatol (NY) 2010; 6: 339-346.
- Malik TA. Inflammatory Bowel Disease: Historical Perspective, Epidemiology, and Risk Factors. The surgical clinics of North America 2015; 95: 1105-1122.
- Hugot JP, Zouali H, Lesage S, Thomas G. Etiology of the inflammatory bowel diseases. International Journal of Colorectal Disease 1999; 14: 2-9.
- Loftus EV, Jr. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence, and environmental influences. Gastroenterology 2004; 126: 1504-1517.
- Lakatos PL. Recent trends in the epidemiology of inflammatory bowel diseases: Up or down? World J Gastroenterol 2006; 12: 6102-6108.
- Shivananda S, Lennard-Jones J, Logan R, Fear N, Price A, Carpenter L, van Blankenstein M. Incidence of inflammatory bowel disease across Europe: Is there a difference between north and south? Results of the European Collaborative Study on Inflammatory Bowel Disease (EC-IBD). Gut 1996; 39: 690- 697.
- Hinojosa J, Primo J, Lledo S, López A, Roig JV, Fernández J. Incidence of inflammatory bowel disease in Sagunto. Rev Esp Enferm Dig 1990; 78: 283-287.
- López-Serrano P, Pérez-Calle JL, Carrera-Alonso E, Pérez-Fernández T, Rodríguez-Caravaca G, Boixeda-de-Miguel D, Fernández-Rodriguez CM. Epidemiologic study on the current incidence of inflammatory bowel disease in Madrid. Rev Esp Enferm Dig 2009; 101: 768-772.
- Yepes Barreto IdJ, Carmona R, Díaz F, Marín-Jiménez I. Prevalencia y características demográficas de la enfermedad inflamatoria intestinal en Cartagena, Colombia. Rev Col Gastroenterol 2010; 25: 107-111.
- Gaburri PD, Chebli JM, de Castro LE, Ferreira JO, Lopes MH, Ribeiro AM, Alves RA, Froede EC, de Oliveira KS, Gaburri AK, Gaburri D, Meirelles GS, de Souza AF. (Epidemiology, clinical features and clinical course of Crohn’s disease: a study of 60 cases). Arq Gastroenterol 1998; 35: 240-246.
- Souza MH, Troncon LE, Rodrigues CM, Viana CF, Onofre PH, Monteiro RA, Passos AD, Martinelli AL, Meneghelli UG. [Trends in the occurrence (1980-1999) and clinical features of Crohn’s disease and ulcerative colitis in a university hospital in southeastern Brazil]. Arq Gastroenterol 2002; 39: 98-105.
- Figueroa CC, Quera PR, Valenzuela EJ, Jensen BC. Inflammatory bowel disease: experience of two Chilean centers. Rev Med Chil 2005; 133: 1295-1304.
- Linares de la Cal JA, Canton C, Hermida C, Pérez-Miranda M, Mate-Jimenez J. Estimated incidence of inflammatory bowel disease in Argentina and Panama (1987-1993). Rev Esp Enferm Dig 1999; 91: 277-286.
- Torres EA, Cruz A, Monagas M, Bernal M, Correa Y, Cordero R, Carlo VL. Inflammatory Bowel Disease in Hispanics: The University of Puerto Rico IBD Registry. International Journal of Inflammation 2012; 2012: 574079.
- Torres EA, De Jesus R, Perez CM, Inesta M, Torres D, Morell C, Just E. Prevalence of inflammatory bowel disease in an insured population in Puerto Rico during 1996. Puerto Rico Health Sciences Journal 2003; 22: 253-258.
- Victoria CR, Sassak LY, Nunes HR. Incidence and prevalence rates of inflammatory bowel diseases, in midwestern of Sao Paulo State, Brazil. Arq Gastroenterol 2009; 46: 20-25.
- Buenavida G, Casañas A, Vásquez C, De Souza M, Martínez L, Gardil I, Silveira A, Iade B. Incidence of inflammatory bowel disease in five geographical areas of Uruguay in the biennial 2007- 2008. Acta Gastroenterol Latinoam 2011; 41: 281-287.
- Instituto Nacional de Estadística de Uruguay. Censo de población y hogares 2004. http://www.ine.gub.uy. 2004.
- Instituto Nacional de Estadística de Uruguay. Encuesta Nacional de Hogares Ampliada 2006. http://www.ine.gub.uy/enha2006/ informestematicos.asp. 2006.
- Instituto Nacional de Estadística de Uruguay. Uruguay en Cifras 2008. http://www.ine.gub.uy/documents/10181/39317/ Uruguay+en+cifras+2008.pdf.
- Farrukh A, Mayberry JF. Inflammatory bowel disease in Hispanic communities: a concerted South American approach could identify the aetiology of Crohn’s disease and ulcerative colitis. Arq Gastroenterol 2014; 5: 271-275.
- da Silva BC, Lyra AC, Mendes CM, Ribeiro CP, Lisboa SR, de Souza MT, Portela RC, Santana GO. The Demographic and Clinical Characteristics of Ulcerative Colitis in a Northeast Brazilian Population. Biomed Research International 2015; 2015: 359130
- Simian D, Fluxa D, Flores L, Lubascher J, Ibanez P, Figueroa C, Kronberg U, Acuna R, Moreno M, Quera R. Inflammatory bowel disease: A descriptive study of 716 local Chilean patients. World J Gastroenterol 2016; 22: 5267-5275.
- Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012; 142: 46-54.
- Bosques-Padilla FJ, Sandoval-García ER, Martinez-Vázquez MA, Garza-González E, Maldonado-Garza HJ. Epidemiología y características clínicas de la colitis ulcerosa crónica idiopática en el noreste de México. Rev Gastroenterol Mex 2011; 76: 34-38.
- Parente JM, Coy CS, Campelo V, Parente MP, Costa LA, da Silva RM, Stephan C, Zeitune JM. Inflammatory bowel disease in an underdeveloped region of Northeastern Brazil. World J Gastroenterol 2015; 21: 1197-1206.
- Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis 2011; 17: 423-439.
- Instituto Nacional de Estadística de Uruguay. Censo de poblacion y hogares 2011. www.ine.gub.uy/web/guest/tematicos. 2011.
Correspondencia: Beatriz Iade
Gastroenterology Clinic, Hospital de Clínicas – Faculty of Medicine UDELAR. Av. Italia SN. Montevideo, Uruguay
Tel.: (5982) 4808472/ (5982) 9081818 / Tel. Cel.: (5989) 962 1367
Correo electrónico: beatriz.iade@gmail.com
Acta Gastroenterol Latinoam 2018;48(3): 154-158
