Alejandro Rey,1 Virginia Margarita Cano Busnelli,2 Juan Pablo Santino,3 Fernando Van Domselaar,4 Guillermo Ojea Quintana,2 Alberto Cristian Seehaus,5 Juan Andrés De Paula1
1 Servicio de Gastroenterología, Hospital Italiano. Ciudad Autónoma de Buenos Aires, Argentina.
2 Servicio de Coloproctología, Hospital Italiano. Ciudad Autónoma de Buenos Aires, Argentina.
3 Servicio de Anatomía Patológica, Hospital Italiano. Ciudad Autónoma de Buenos Aires, Argentina.
4 Servicio de Gastroenterología, Hospital Regional de Comodoro Rivadavia. Chubut, Argentina.
5 Servicio de Diagnóstico por Imágenes, Hospital Italiano. Ciudad Autónoma de Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2016;46:43-47
Recibido: 03/05/2015 / Aprobado: 09/11/2015 / Publicado en www.actagastro.org el 31/03/2016

Summary
Mesenteric lipodystrophy is a rare inflammatory process that predominantly affects mesenteric adipose tissue of the small bowell. Several mechanisms have been suggested as responsible for this entity although the precise etiology remains unknown. The diagnosis is based on CT or MRI imaging and generally confirmed by surgical biopsies. Treatment is individualized and empiric and depends on disease stage and symptoms. We report a case of a 35-year-old male who was admitted to our hospital with a history of abdominal pain, constipation and a palpable mass in the left lower quadrant. Abdominal CT scan showed diffuse thickening of the descending and rectosigmoid colon, associated with increased density of the mesenteric fat. After failure of an initial treatment with glucocorticoids, he underwent a laparoscopic sigmoidectomy. Histopathology analysis revealed extensive steatonecrosis of pericolonic fat and lipid-laden foamy cells which was consistent with the diagnosis of mesenteric lipodystrophy. Clinical presentation and treatment as well as a brief review of the literature are discussed.
Key words. Mesenteritis, lipodystrophy; panniculitis; sclerosing mesenteritis, colon.
Lipodistrofia mesenterica extensa de colon izquierdo: reporte de caso y breve revisión de la literatura
Resumen
La lipodistrofia mesentérica es un proceso inflamatorio infrecuente que afecta predominantemente el tejido adiposo del peritoneo del intestino delgado. Pese a que diversos mecanismos han sido sugeridos como responsables de esta entidad, la etiología precisa permanece desconocida. El diagnóstico se basa en las imágenes obtenidas por tomografía computada o resonancia magnética y generalmente es confirmado a partir de biopsias quirúrgicas. El tratamiento es individualizado y empírico, y depende del estadio de la enfermedad y la sintomatología. Reportamos el caso de un hombre de 35 años que fue ingresado a nuestro centro presentando dolor abdominal, constipación y una masa palpable en la fosa ilíaca izquierda. La tomografía computada de abdomen mostró engrosamiento difuso del colon descendente y rectosigmoide asociado al incremento de la densidad de la grasa mesentérica. Luego del fracaso del tratamiento inicial con glucocorticoides, se realizó una sigmoidectomía laparoscópica. El estudio histopatológico de la pieza quirúrgica reveló extensa esteatonecrosis de la grasa peri colónica y macrófagos espumosos cargados de lípidos, hallazgos compatibles con lipodistrofia mesentérica. La presentación clínica y el tratamiento, al igual que una breve reseña de la literatura actual, se discuten a continuación.
Palabras claves. Mesenteritis, lipodistrofia, paniculitis, mesenteritis esclerosante, colon.
Abreviatures
CEA: carcinoembrional antigen.
CT: computed tomography.
IgG: immunoglobulin G.
MRI: magnetic resonance imaging.
Mesenteric lipodystrophy is part of a spectrum of primary idiopathic inflammatory and fibrotic processes affecting mesenteric adipose tissue.1 Since the original description by Jura in 1924 under the term “retractile mesenteritis”, and later in the 1960 by Odgen as “mesenteric panniculitis”, several other denominations have been used to describe conditions presenting with overlapping clinical and histologic features, including mesenteric lipodystrophy and sclerosing mesenteritis.1, 2
Although histologic progression has rarely been documented, most patients present a range of pathology findings with one salient or predominant feature. These may represent different phases in the natural course of the underlying process, evolving from adipocyte necrosis (mesenteric lipodystrophy) to a chronic inflammatory state (mesenteric panniculitis), and finally to fibrosis (sclerosing mesenteritis).3
Despite being an extremely rare condition, a number of reports have been published in recent years, suggesting increased interest in this clinical entity.1, 2, 4-6 Having obtained consent from the patient, we present an unusual case of mesenteric lipodistrophy with extensive steatonecrosis of the pericolonic fat of the descending and rectosigmoid colon, and look forward to contribute with useful information for future studies and research.
Case report
A 35-year-old male physician, who worked as an intensivist at a regional hospital, was admitted to our center with a 2-week history of lower left abdominal pain, moderate to severe in intensity, with intermittent abdominal cramps, associated with severe constipation, mucorrhea and a palpable mass in the left lower quadrant. Patient had no fever, and referred no nausea or vomiting. Except for laparoscopic appendectomy 3 years earlier, his past medical history was unremarkable. Patient was not receiving any form of medication.
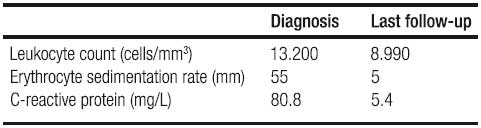
Physical examination revealed a tender palpable mass in the left lower quadrant of the abdomen with no signs of peritonitis. Vital signs were stable and patient was otherwise in good general condition. Laboratory results indicated: leukocytosis (13.200 cells/mm3), elevation in erythrocyte sedimentation rate and C-reactive protein (55 mm and 80,8 mg/L and respectively). Red cell count, liver function tests and serum electrolytes were all within normal limits as well as rheumatology markers, CEA, CA 19-9, IgG-4 and urine tests.
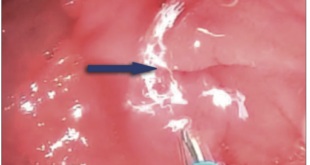
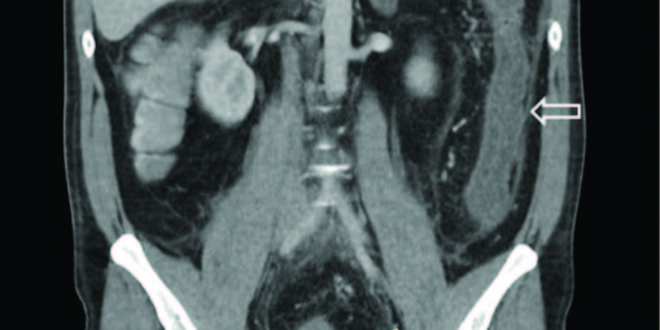
Abdominal multislice CT scan with oral and intravenous contrast showed diffuse thickening of the descending and rectosigmoid colon, associated with increased density of the mesenteric fat, enlarged mesenteric vessels and a small amount of free abdominal fluid, suggesting presence of an inflammatory condition (Figure 1). Left-sided colonoscopy was performed with a Pentax EPK-P processor and EC-380 LKP colonoscope, revealing signs of ischemia in the descending and rectosigmoid colon: mucosal erythema and edema, reduced bowel lumen and rigid walls. Transverse colon and lower rectum were spared.
Figure 1. Abdominal multislice CT scan: diffuse thickening of the descending and rectosigmoid colon (large arrow), associated with an increase in density of the mesenteric fat and a small amount of free abdominal fluid (small arrow).

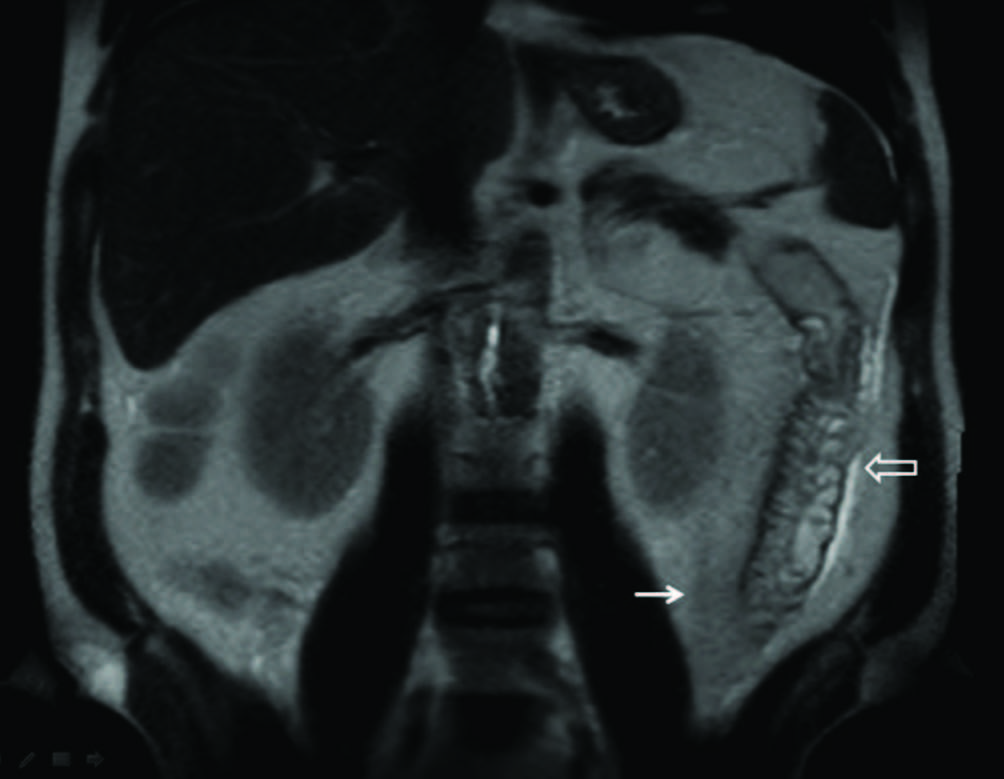
Suspecting a primary inflammatory disorder involving the adipose tissue of the mesentery, treatment was started with prednisone 40 mg once daily. Initial response consisted in scarce liquid stools and bloody mucus without significant variations in blood parameters regarding inflammation. After five days, the patient continued suffering from abdominal pain and constipation without passage of flatus. Abdominal MRI revealed inflammatory changes of the mesentery and persistence of bowel wall thickening with submucosal edema (Figure 2).
On the basis of these findings, abdominal surgery was indicated. Exploratory laparotomy revealed pathological mesenteric fat infiltrated by dense tissue. Rigidity of the sigmoid colon and superior rectum impaired mobilization. All involved segments appeared covered by fibrin and adhered to mesenteric vessels, as well as to retroperitoneal fat and to the left urether. Digital palpation confirmed rectum was edematous and stiff and mesorrectum hardened. Sigmoidectomy with resection of the upper rectum was performed and closure of the rectal stump accomplished using mechanical suture. An end colostomy was created. Patient had an uneventful postoperative recovery and was discharged four days later.
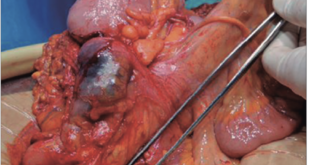
Visual examination of the surgical specimen showed marked thickening of sigmoid colon and rectum mesentery, with areas of focal congestion, hemorrhage and fibrin deposits. Normal adipose tissue architecture was altered and replaced by an irregular nodular mass with necrotic areas (Figure 3). Linear ulcers were observed along the mucosa which presented edematous changes.
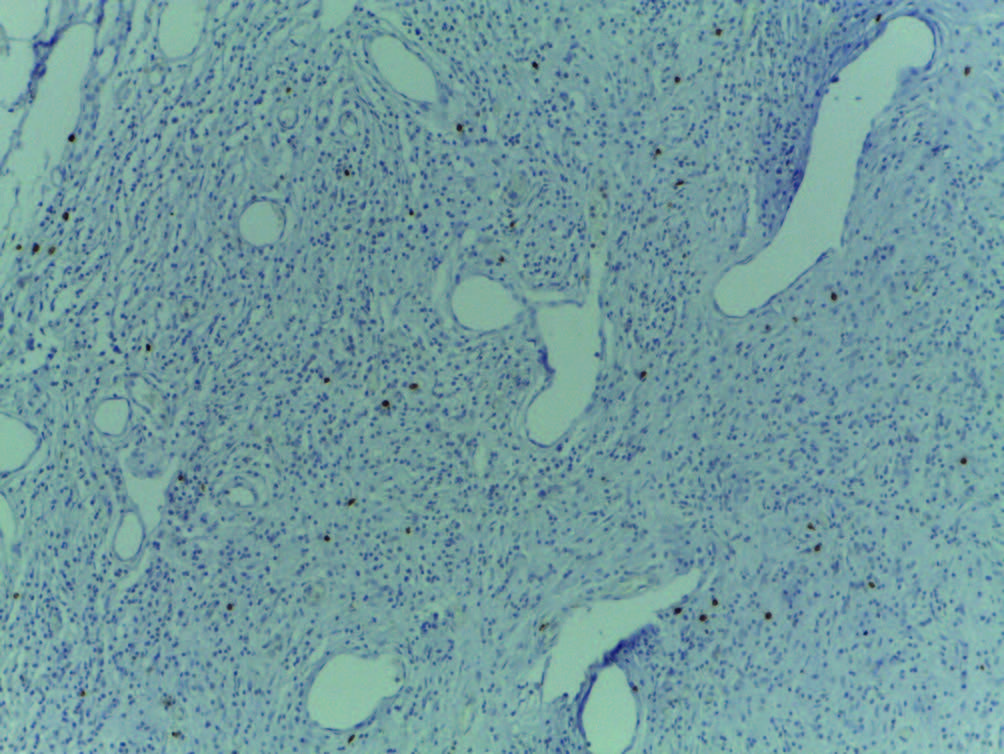
Histopathology of microscopic sections revealed extensive steatonecrosis of pericolonic fat, presence of lipid-laden foamy cells and scattered areas of fibrosis, all of which led to the diagnosis of mesenteric lipodistrophy (Figure 4). Mild lymphocyte and plasma cell infiltration was present. The rectosigmoid colon wall showed inflammatory changes associated with erosion of the mucosa. No evidence of vasculitis or neoplasia was observed.

Four months after the first intervention, the patient underwent a laborious reconstructive surgery requiring complete resection of the remaining rectum and mesorectum with coloanal anastomosis due to peritoneal adherences. The surgical piece showed disease-free margins. The patient achieved full recovery, normalization of blood tests and remains asymptomatic at present (Table 1). In consent with him, no other medication was prescribed and active surveillance was decided. For the time being, he remains without clinical or imagenological manifestations of disease relapse.
Table 1. Inflammatory state at diagnosis and last follow-up.
Discussion
Mesenteric lipodystrophy is an extremely uncommon non neoplastic inflammatory process of the mesenteric fat, predominantly affecting white Caucasian males in the fifth to seventh decades of life, although cases have been reported between the ages of 20 and 80 years.1, 2
Several mechanisms have been suggested as responsible for this entity, mostly based on case reports, small case series or extrapolation of data from animal models of inflammation; however, the precise etiology remains unknown. A nonspecific response to a wide variety of stimuli including vasculitis and autoimmune disorders, malignancies, ischemia, bacterial infection and abdominal trauma or surgery seems one possible explanation.3, 4 Moreover, recent findings suggest some cases diagnosed as mesenteric lipodystrophy may actually be a subset of IgG4-related sclerosing disorders.7
The disease predominantly affects the mesentery of the small intestine and rarely involves the large bowel.8 According to a literature review by Karentzos et al in 1990, only 5 of 124 cases of mesenteric lipodystrophy involved the sigmoid colon mesentery.9 In another review of 52 cases of retractile mesenteritis of the large bowel by Ikoma et al. in 1996, isolated involvement of the mesocolon was found in 20% of cases, with the rectosigmoid as the most common site affected.10
Mesenteric lipodystrophy is generally asymptomatic and often incidental. When symptomatic, clinical features may be progressive or intermittent and usually non-specific.4 Patients can present with abdominal tenderness or a palpable abdominal mass, protein-losing enteropathy with diarrhea or bowel disturbance of variable duration, accompanied by systemic manifestations such as weight loss, fatigue and fever of unknown origin. Laboratory findings are also usually non-specific and may include elevation of erythrocyte sedimentation rate and C-reactive protein level, leukocytosis and anemia.1, 4, 6 Additionally, in the case we describe, fibro-inflammatory involvement of mesocolonic adipose tissue may have been responsible for a reduction in blood flow with subsequent hypoperfusion of the mesenteric vasculature and non-occlusive ischemia.
Despite its limited specificity, dual-phase abdominal CT is the most sensitive imaging modality for detecting mesenteric lipodystrophy. The most common CT finding is a soft tissue mass in the small bowel mesentery, which may be either homogeneous or heterogeneous depending upon the extent and severity of fibrosis and inflammation, respectively.11 Less frequently, increased attenuation of mesenteric fat with small lymph nodes, but without evidence of a discrete mass (“misty mesentery”) has been described, although not a specific sign of the disease.12 Two CT findings are considered to have a certain degree of specificity for mesenteric lipodystrophy. The “fat ring sign”, which describes the preservation of the densitometric values of fat nearest the mesenteric vessels, is seen in 75 to 90 percent of patients. The “tumoral pseudocapsule”, present in up to 60 percent of patients, refers to the image of a hyperattenuated stripe partly surrounding the mass.13, 14 Vascular encasement, displacement, or thrombosis can be seen in over 50% of the cases.15 MRI findings appear to be similar to CT although it has been less extensively studied.16 Plain radiographs and ultrasonographic studies are less useful and generally inconclusive for diagnosis and PET/CT scanning findings remain controversial because of contradictory results.17-19
Microscopically, lipodystrophy is initially characterized by mesenteric infiltration by lipid-filled macrophages into the septa of the adipose tissue, with little or no sign of acute inflammation. As inflammation progresses, lymphocytic infiltration develops together with lipid cystic necrosis, corresponding to the second stage known as panniculitis. Finally, collagen deposits and fibrosis are observed at the end-stage of disease, known as retractile mesenteritis.1, 2 These histological findings are generally sufficient to provide diagnosis, but in more difficult cases, immunochemistry might prove useful to distinguish it from other differential diagnoses.1, 7
No standard therapy has been recommended for mesenteric lipodystrophy.6 Empiric individualized treatment depends on disease stage and symptoms, and is based on published case reports and small case series. In the early stages, mesenteric lipodystrophy tends to resolve spontaneously without treatment, although its behavior can be unpredictable. As chronic inflammation progresses but prior to the development of fibrosis, a number of pharmaceutical agents have been used in an attempt to stabilize the disease.5 Glucocorticoids alone or in combination with tamoxifen, colchicine, thalidomide, cyclophosphamide, or azathioprine have been reported to be beneficial, as well as oral treatment with progesterone.1, 4, 8, 20 Beyond diagnostic sampling, surgery may become necessary in the final stages if medical therapy fails, or in the presence of complications such as bowel obstruction or perforation.3, 5
We report a case of a young patient with unusual and extensive idiopathic mesenteric lipodystrophy of the descending and rectosigmoid colon, who presented with a palpable mass in the left abdomen accompanied by signs of colonic ischemia and partial bowel obstruction of rapid onset. The aggressiveness of the disease and the lack of response to systemic therapy ultimately required extensive and demanding two-stage surgical excision of the affected segment. Our case illustrates that mesenteric lipodystrophy is not always a slowly progressive, benign and chronic condition, but can be an aggressive disease, with rapid onset of signs and symptoms and challenging management.
Conflict of interests. The authors state there is no conflict of interest.
References
- Issa I. Mesenteric panniculitis: Various presentations and treatment regimens. World J Gastroenterol 2009; 15: 3827.
- Vettoretto N, Diana DR, Poiatti R, Matteucci A, Chioda C. Occasional finding of mesenteric lipodystrophy during laparoscopy : A difficult diagnosis. World J Gastroenterol 2007; 13: 5394-5396.
- Emory TS, Monihan JM, Carr NJ, Sobin LH. Sclerosing mesenteritis, mesenteric panniculitis and mesenteric lipodystrophy: a single entity? Am J Surg Pathol 1997; 21: 392-398.
- Gunduz Y, Tatli APL, Kara RO. Mesenteric panniculitis: a case report and review of the literature. Mædica 2012; 7: 344-347.
- Chawla S. An unusual presentation of sclerosing mesenteritis as pneumoperitoneum: Case report with a review of the literature. World J Gastroenterol 2009; 15: 117.
- Nobili C, Degrate L, Caprotti R, Franciosi C, Leone BE, Romano F, Dinelli M, Uggeri F. Extensive sclerosing mesenteritis of the rectosigmoid colon associated with erosive colitis. Gastroenterol Res Pract 2009; 2009: 176793.
- Chen TS, Montgomery E a. Are tumefactive lesions classified as sclerosing mesenteritis a subset of IgG4-related sclerosing disorders? J Clin Pathol 2008; 61: 1093-1097.
- Wexner SD, Attiyeh FF. Mesenteric panniculitis of the sigmoid colon. Report of two cases. Dis Colon Rectum 1987; 30: 812-815.
- Karentzos S, Tzoutzos D, Stavropoulos G, Giannakou N, Gkiconti I, Giannakakis A. [Mesenteric panniculitis of the sigmoid. A case report and review of the literature]. Minerva Chir 1990; 45: 1403-1406.
- Ikoma A, Tanaka K, Komokata T, Ohi Y, Taira A. Retractile mesenteritis of the large bowel: report of a case and review of the literature. Surg Today 1996; 26: 435-438.
- Daskalogiannaki M, Voloudaki A, Prassopoulos P, Magkanas E, Stefanaki K, Apostolaki E, Gourtsoyiannis N. CT evaluation of mesenteric panniculitis: prevalence and associated diseases. AJR Am J Roentgenol 2000; 174: 427-431.
- McLaughlin PD, Filippone A, Maher MM. The “misty mesentery”: Mesenteric panniculitis and its mimics. Am J Roentgenol 2013; 200: 116-123.
- Patel N, Saleeb SF, Teplick SK. General case of the day. Mesenteric panniculitis with extensive inflammatory involvement of the peritoneum and intraperitoneal structures. Radiographics 1999; 19: 1083-1085.
- Horton KM, Lawler LP, Fishman EK. CT findings in sclerosing mesenteritis (panniculitis): spectrum of disease. Radiographics 2003; 23: 1561-1567.
- Lawler LP, McCarthy DM, Fishman EK, Hruban R. Sclerosing mesenteritis: depiction by multidetector CT and three-dimensional volume rendering. AJR Am J Roentgenol 2002; 178: 97-99.
- Kobayashi S, Takeda K, Tanaka N, Hirano T, Nakagawa T, Matsumoto K. Mesenteric panniculitis: MR findings. J Comput Assist Tomogr 1993; 17: 500-502.
- Zissin R, Metser U, Hain D, Even-Sapir E. Mesenteric panniculitis in oncologic patients: PET-CT findings. Br J Radiol 2006; 79: 37-43.
- Pérez-Fontán FJ, Soler R, Sánchez J, Iglesias P, Sanjurjo P, Ruiz J. Retractile mesenteritis involving the colon: barium enema, sonographic, and CT findings. AJR Am J Roentgenol 1986; 147: 937-940.
- Nguyen BD. F-18 FDG PET demonstration of sclerosing mesenteritis. Clin Nucl Med 2003; 28: 670-671.
- Mazure R, Fernandez Marty P, Niveloni S, Pedreira S, Vazquez H, Smecuol E, Kogan Z, Boerr L, Mauriño E, Bai JC. Successful treatment of retractile mesenteritis with oral progesterone. Gastroenterology 1998; 114: 1313-1317.
Correspondence: Alejandro Rey
Servicio de Gastroenterología, Hospital Italiano de Buenos Aires, Gascón
450, 1181, Ciudad Autónoma de Buenos Aires, Argentina.
Tel: +54-114959-0200 int 8862 Fax: +54-114959-0200 int 8249
Correo electrónico: alejandro.rey@hospitalitaliano.org.ar
Acta Gastroenterol Latinoam 2016;46(1):43-47