María Soledad Rubio Mainardi, Álvaro Alcaraz, Saleg Patricia, María Eugenia Romero, Federico Moser, Lucio Ricardo Obeide
Departamento de Cirugía General del Hospital Privado de Córdoba. Córdoba, Argentina.
Acta Gastroenterol Latinoam 2015;45:320-322
Recibido: 29/03/2015 / Aprobado: 10/07/2015 / Publicado en www.actagastro.org el 30/12/2015

Summary
Background. Metallic stent placing is the first choice in the treatment of malign or benign strictures of the esophagus. Stent migration is a well-known complication of this procedure. We report a case of stent migration in which surgical laparoscopic intervention was used to retrieve it. Methods. An 85 years old man with unsuccessfully endoscopic retrieval of a migrated stent underwent laparoscopic gastrotomy for solution. The patient recovered without incident. Conclusion. This case illustrates that laparoscopic technique can be an optional way to retrieve migrated stents in selected patients.
Key words. Stent migration, stent complications, laparoscopic technique, esophageal cancer.
Migración de un stent esofágico. Caso clínico sobre la recuperación de un stent movido
Resumen
Antecedentes. La colocación de un stent metálico es la primera opción en el tratamiento de las estenosis malignas o benignas del esófago. La migración del stent es una complicación bien conocida de este procedimiento. Se presenta un caso de migración del stent en el que se utilizó la intervención quirúrgica laparoscópica para recuperarlo. Métodos. Un hombre de 85, años en el que se realizó sin éxito una endoscopía para intentar la recuperación de un stent migrado, fue sometido a una gastrostomía laparoscópica para su recuperación. El paciente se recuperó sin complicaciones. Conclusión. Este caso ilustra que la técnica laparoscópica puede ser una forma opcional para recuperar stents migrados en pacientes seleccionados.
Palabras claves. Migración de stent, complicación de stent, técnica laparoscópica, cáncer esofágico.
Self-expanding metal stent placement has been the first choice for palliative therapy of the unresectable esophageal cancer.1 These stent are also highly effective for the management of benign (peptic, postsurgical, corrosive) strictures refractory to dilation, esophageal leaks, perforations and fistula. In most cases rapid relief of disphagia and adequate oral intake of nutrients can be achieved. Although complications at the time of insertion are not uncommon, most stent can successfully be managed by experienced endoscopists and only a few of them are lethal.2
Removal of migrated stent in the stomach is recommended to avoid gastrointestinal complications such as bleeding, obstruction and perforation.3, 4 Sometimes, this can be technically challenging and can’t be retrieved by endoscopy.
In this paper we present a case of stent migration not removed by endoscopy that was retrieved by laparoscopic gastrostomy.
Case report
An 85 years old man was diagnosed six months ago with unresectable esophageal cancer and in the last weeks started complaining about intolerable disphagia and cough. Endoscopic examination revealed a stenosis in the distal esophagus that was stented with silicon coated wall stent (25 mm diameter, 10 cm length).
At the time of insertion, the stent migrated into the stomach. The patient was asymptomatic but surgical consult was done as recommended after unsuccessfully endoscopic retrieval.
Although alternatives and risks, we decided to perform a laparoscopic gastrostomy for retrieval of the foreign body.
Pneumoperitoneum was established with an open technique at the supraumbilical crease. A 10 mm port was placed there and, by direct visualization, a 5 mm port a two 10 mm ports where placed in the epigastria, in the left subcostal area and right subcostal area respectively. The first 10 mm port was changed for a 15 mm port for mechanical suture.
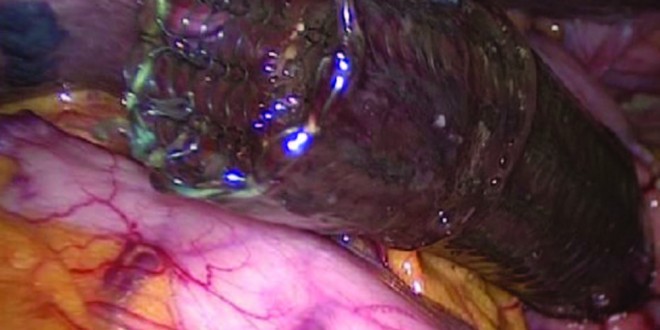
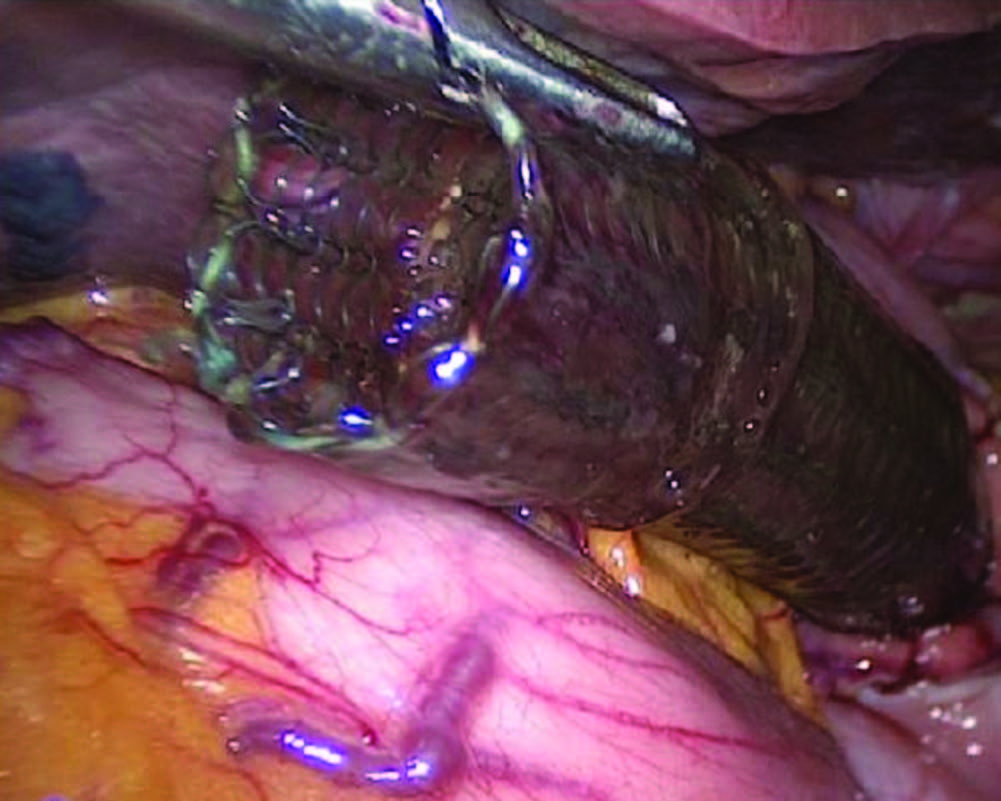
A gastrostomy about 2 cm in length was made over the stomach antrum and after aspiration we introduced the laparoscope into the stomach where the stent was noted sitting in the fundus.
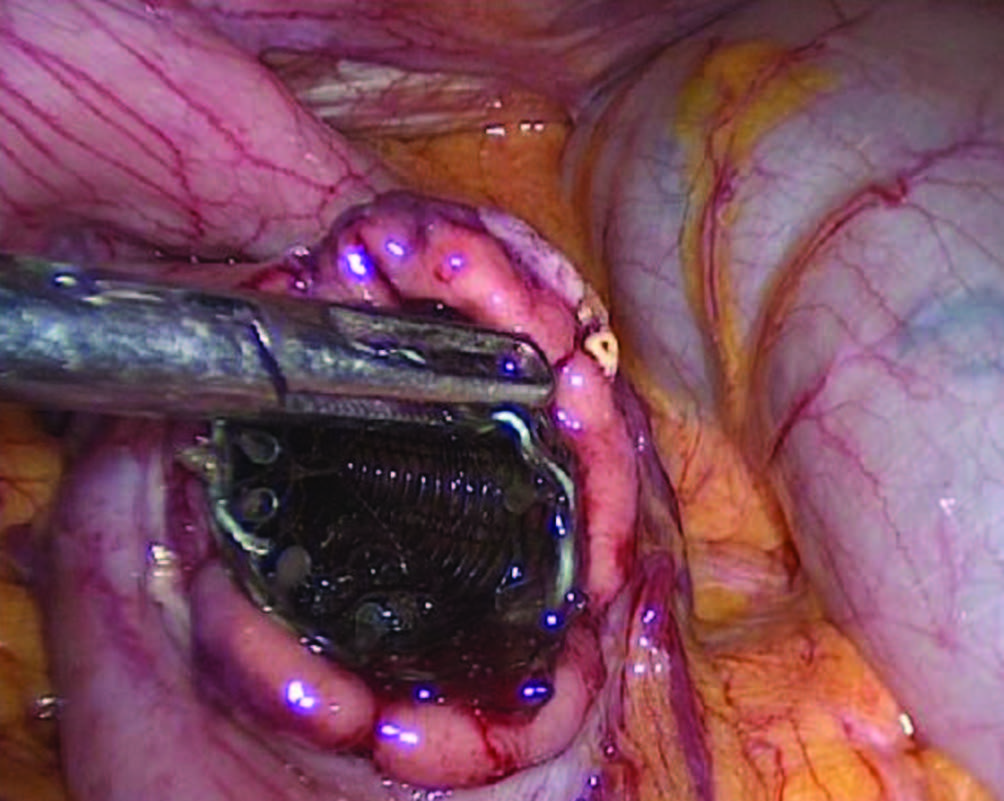
The dislodged stent was withdrawn with a laparoscopic forceps and placed into a plastic bag which was now withdrawn from abdomen through the 10 mm left incision.
The gastrostomy was closed using a endoGIA stapling device via the 15 mm port.
After closure of the gastrostomy, peritoneal lavage was done, a nasogastric tube was left in place in the stomach for decompression and a silicon multilumen drainage was placed in the major curvature.
The 15 mm port site and the 10 mm right port site were closed using a 1-vicryl suture.
Oral intake was started 36 hs from surgery and hospital discharged 72 hs from it. No complications were registered.
Patient died four months later because of primary cancer ingrowth.
Briefly, stent migrations have to be considered as a potential life threatening complication and symptomatic or not, should be followed closely or removed immediately, indication where laparoscopy can be the first choice.
Discussion
Self expanding metallic stents are widely employed to relieve malignant esophageal obstruction because they are easy to use, relatively safe and effective in allowing patients to consume a normal diet.5, 6
Covered metallic stent are coated with silicon and avoid ingrowth of tumor through the metal mesh. In this case the patient has a covered stent.
Migration of the deployed stent is one of the most common complications. Coated stent are more likely to migrate. Stent placed for tumors of the distal esophagus or gastric cardia is more likely to migrate too. Therefore stent migration has been reported to occur in up to 28% of patients treated with covered stent.10-12
Non surgical removal of dislodged stents is usually difficult and dangerous. If it’s not possible the removal by endoscopy, the surgical consult is recommended. Endoscopist doctors tried on several occasions and endoscopic extraccion but never remove the stent of the stomach, because technical difficulties. So it were decided to performed a lapaparoscopic extraction.
While it was a palliative patient, her performance status was good and once diagnosed was performed we decided remove the stent to avoid the risk of bleeding, obstruction or perforation.
Avoiding the morbidity associated with a laparotomy and open gastrostomy by a laparoscopic technique is a new and accesible option for this patients. We present this case solved by laparoscopic gastrostomy and closed with mechanical suture.
Conclusion
Briefly, stent migrations have to be considered as a potential life threatening complication and symptomatic or not, should be followed closely or removed immediately, indication where laparoscopy can be the first choice.
References
- Knyrim K, Wagner HJ, Bethge N, Keymling M, Vakil N. A controlled trial of an expansible metal stent for palliation of esophageal obstruction due to inoperable cancer. N Engl J Med 1993; 329: 1302-1307.
- May A, Gossner L, Feess G, Bauer R, Ell C. Extraction of migrated self-expanding esophageal metal stents. Gastrointest Endosc 1999; 49: 524-526.
- Oguzhan K, Ersin A, Merith A, Muharrem B, Gokhan A, Servet K. Esophageal stent migration can lead to intestinal obstruction. North Am J Med Sciences 2009; 1: 63-65.
- Harries R, Campbell J, Ghosh S. Fractured migrated esophageal stent fragment presenting as small bowel obstruction three years after insertion. Ann R Coll Surg Engl 2010; 92.
- Sanyal A, Maskell GF, Hohle R, Murray A. An unusual complication of oesophageal stent deployment. British J of Radiology 2006; 79: e103-e105.
- Bravo Pérez JC, Oleaga J. Extracción percutánea, vía tracto de gastrostomía, de un stent esofágico migrado a estómago. Presentación de un caso y revisión del tema. Intervencionismo 2009; 9: 160-163.
- Chander RK, Samuel K, Katz V, Ingram M. Combined laparoscopy and transabdominal endoscopy: case report of dislodged oesophageal stent retrieval. J Min Access Surg 2001; 7: 158-160.
- Reddy VM, Sutton CD, Miller AS. Terminal ileum perforation as a consequence of a migrated and fractured oesophageal stent. Case Rep Gastroenterol 2009; 3: 61-66.
- Adam A, Morgan R, Ellul J, Mason RC. A new design of the esophageal wallstent endoprosthesis resistant to distal migration. AJR 1998; 170: 1477-1481.
- Yang HS, Zhang LB, Wang TW, Zhao YS, Liu L. Clinical application of metallic stents in treatment of esophageal carcinoma. World J Gastroenterol 2005; 11: 451-453.
- Molina-Infante J, Fernández-Bermejo M, Perez-Gallardo B. Removal of a migrated covered metallic stent through an esophageal stricture, with multiple endoloops. Endoscopy 2010; 42: E268- E269.
- Dinani AM, Cortes RA, Sridhara S, Reichert S, Somnay K. Retrieval of a migrated Poliflex stent- a novel technique. Endoscopy 2009; 41: E304-E305.
Correspondencia: Álvaro Alcaraz
Independencia 415 2 A (CP 5000). Córdoba, Argentina
Correo electrónico: alvaroalcaraz@hotmail.com
Acta Gastroenterol Latinoam 2015;45(4):320-322
