Rodolfo Pizarro1 ID· Leandro Barbagelata2 ID
1 Jefe de Cardiología Hospital Italiano de Buenos Aires. Master en Efectividad Clínica.
2 Médico cardiólogo. Staff de cardiologia, Hospital Italiano de Buenos Aires.
Ciudad Autónoma de Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2025;55(4):270-272
Recibido: 05/11/2025 / Aceptado: 05/12/2025 / Publicado online: 23/12/2025 / https://doi.org/10.52787/agl.v55i4.560

En su definición clásica, un confundidor es una variable asociada tanto con la exposición como con el resultado, aunque no está en la línea causal. Esto podría generar asociaciones espurias u ocultar asociaciones existentes. Por ejemplo, un estudio que investiga la asociación entre la hipertensión y el riesgo de insuficiencia cardíaca debería considerar el sobrepeso de los participantes, un predictor independiente de insuficiencia cardíaca (ICC) que probablemente esté asociado con la hipertensión arterial. (Figura 1)
Idealmente, la confusión debería controlarse durante el diseño del estudio. En un ensayo clínico aleatorizado (ECA), por ejemplo, el objetivo de la aleatorización es evitar que las terceras variables de interés se desequilibren por la asignación del tratamiento, reduciendo así la posible confusión. En un estudio poblacional o en entornos clínicos donde la aleatorización no es factible o ética, la confusión puede mitigarse mediante el ajuste multivariable en los modelos de regresión o con enfoques modernos alternativos en la inferencia causal (ejemplo: propensity score).
Figura 1. La relación entre la HTA (exposisión) y el riesgo de IC (variable de resultado) puede confundirse por el sobrepeso (confundidor) que es un factor de riesgo de desarrollar IC y posiblemente asociado a la hipertensión
Es necesario diferenciar el concepto de confundidor, ya explicado, del concepto de la modificación de efecto.
Un modificador del efecto es una tercera variable cuya presencia modifica la fuerza de asociación entre la exposición de interés y el resultado. A diferencia de la confusión, la modificación de efecto no debe ajustarse ni eliminarse, sino describirse.
En el ejemplo previo, la diabetes puede modificar el efecto en la relación de la HTA y la ICC ya que puede ser diferente en aquellos con y sin diabetes (DBT). Desde el punto de vista analítico, se puede detectar modificación de efecto al presentar los resultados en forma estratificada por nivel de la variable modificadora de efecto (ej. diabéticos y no diabéticos), incluyendo un término de interacción en el modelo de regresión. Esto se hace incluyendo el producto del modificador de efecto y la variable de exposición principal (en nuestro ejemplo: HTA x Diabetes), que tendrá un p valor estadísticamente significativo. (Figura 2)
Figura 2. La DBT puede actuar como un modificador de efecto en la relación entre la HTA y la IC; si la estratificamos y hay diferencias entre los DBT y no DBT estamos ante un modificador de efecto de esta relación
Lo podemos ejemplificar de la siguiente manera: Análisis univariado de la relación entre la HTA y el riesgo de ICC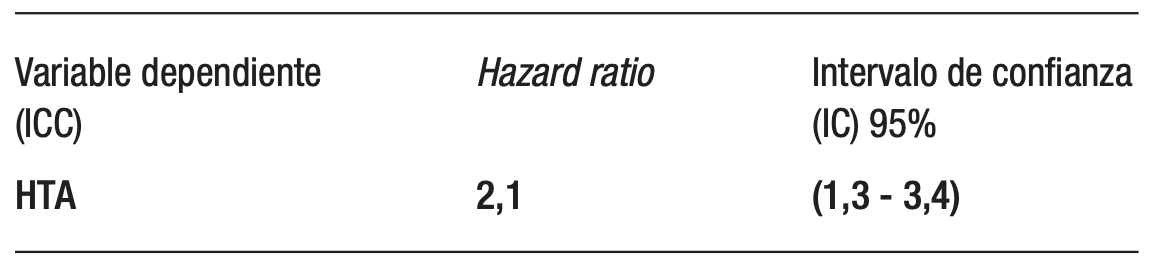
Incorporamos la variable sobrepeso (análisis univariado)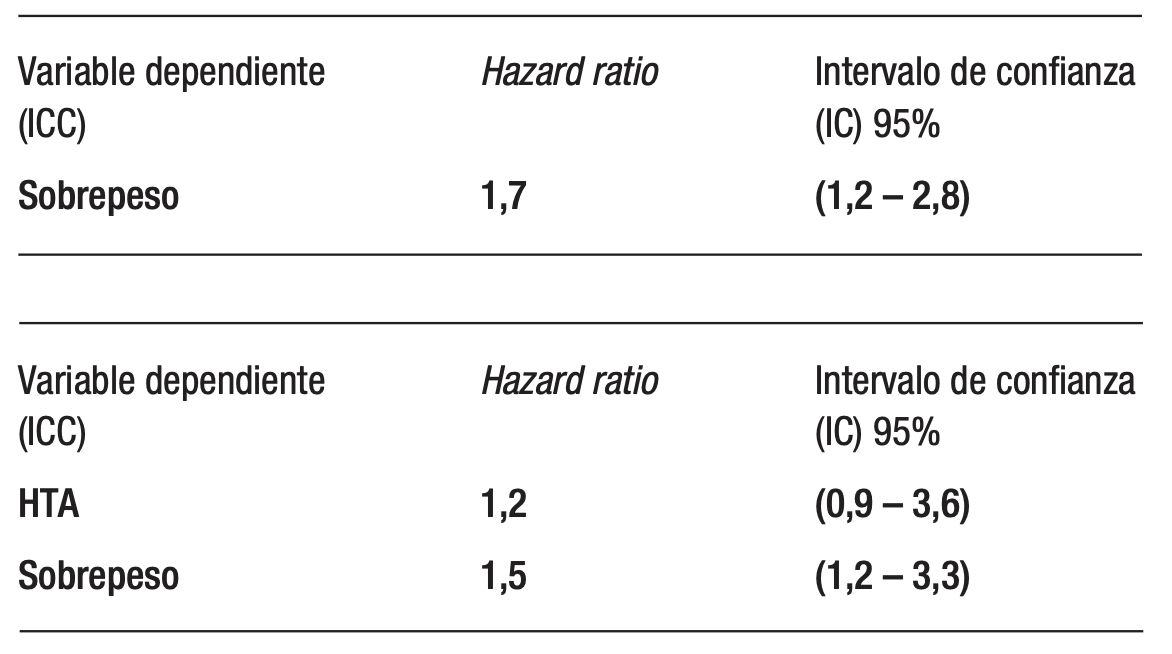
La relación entre la HTA y el riesgo de ICC se altera (el Hazard ratio de la relación univariada se atenúa al ajustar por sobrepeso (2,1 a 1,2) y el intervalo de confianza es menor a 1; no estadísticamente significativo) por la presencia de una segunda variable (sobrepeso), por lo tanto es un confundidor de la relación entre HTA e ICC.
Si estratificamos por la presencia o no de DBT: Pacientes con diabetes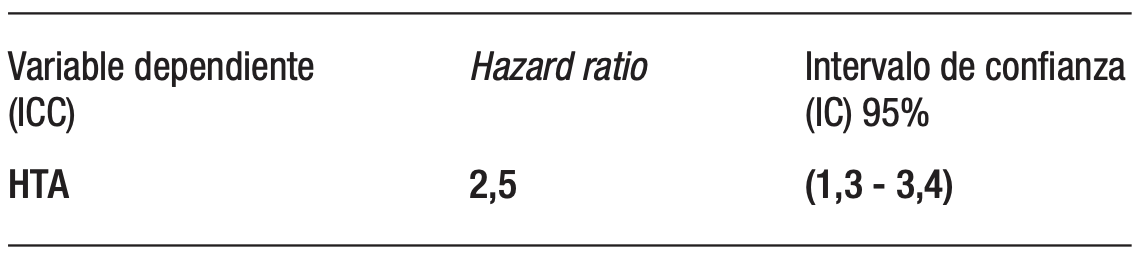
Pacientes sin diabetes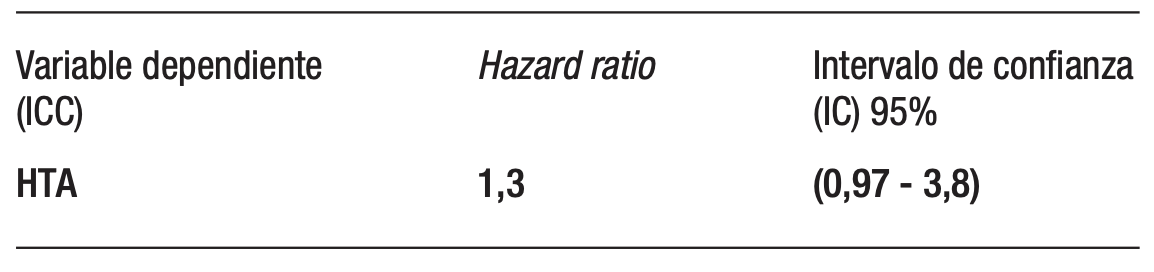
Como vemos, la relación entre HTA e ICC es diferente según lo estratificamos por la presencia o ausencia de DBT (modificador de efecto); también podemos incorporar el producto de la interacción de DBT x HTA en el modelo multivariado de ICC.
El concepto de confundidor es de importancia clave en estudios observacionales en los que se pretende evaluar causalidad, ya que al no estar equilibradas las características basales de los participantes entre los grupos (randomización) hay que ajustar por ellas.
En estudios observacionales, la confusión es una fuente de sesgo que debe controlarse mediante diseño o análisis, mientras que la modificación de efecto representa una heterogeneidad real del efecto entre subgrupos y debe describirse. Distinguir confusión y modificación de efecto es un requisito para una adecuada interpretación causal.
Propiedad intelectual. Los autores declaran que los datos y las tablas presentes en el manuscrito son originales y se realizaron en sus instituciones pertenecientes.
Financiamiento. Los autores declaran que no hubo fuentes de financiación externas.
Conflictos de interés. Los autores declaran no tener conflictos de interés en relación con este artículo.
Aviso de derechos de autor

© 2025 Acta Gastroenterológica Latinoamericana. Este es un artículo de acceso abierto publicado bajo los términos de la Licencia Creative Commons Attribution (CC BY-NC-SA 4.0), la cual permite el uso, la distribución y la reproducción de forma no comercial, siempre que se cite al autor y la fuente original.
Cite este artículo como: Pizarro R y Barbagelata L. Confundidores y Modificadores de Efecto. Acta Gastroenterol Latinoam. 2025;55(4):270-272. https://doi.org/10.52787/agl.v55i4.560
Bibliografía
Bellavia A, Murphy SA. Confounders, Effect Modifiers, and Mediators: Dealing With “Third Variables” in Cardiovascular Epidemiology. Circulation 2025;151:1755-1757.
Lee H, Cashin AG, Lamb SE, Hopewell S, et al.; AGReMA Group. A guideline for reporting mediation analyses of randomized trials and observational studies: the AGReMA statement. JAMA. 2021;326:1045-1056.
Jager KJ, Zoccali A, McLeod A, Dekker FW. Confounding: What it is and how to deal with it. Kidney International 2008;73:256-260.
Kiriakou DN, Lewis DJ. Confounding by indication in clinical research. JAMA 2016;316:1818-1819.
Desai RJ, Franklin JM. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: a primer for practitioners. BMJ 2019;367:l5657.
Correspondencia: Leandro Barbagelata
Correo electrónico: leandro.barbagelata@hospitalitaliano.org.ar
Acta Gastroenterol Latinoam 2025;55(4):270-272
Confounders and Effect Modifiers
Rodolfo Pizarro1 ID· Leandro Barbagelata2 ID
1 Head of Cardiology, Hospital Italiano de Buenos Aires. Master in Clinical Effectiveness.
2 Cardiologist. Cardiology staff, Hospital Italiano de Buenos Aires.
City of Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2025;55(4):273-275
Received: 05/11/2025 / Accepted: 05/12/2025 / Published online: 23/12/2025 / https://doi.org/10.52787/agl.v55i4.560
According to the classic definition, a confounder is a variable that is associated with both the exposure and the outcome, although it is not on the causal pathway. This could generate spurious associations or obscure existing ones. For instance, a study investigating the association between hypertension and heart failure risk should consider overweight participants, an independent predictor of heart failure (HF) that is likely associated with high blood pressure. (Figure 1)
Ideally, confounding factors are controlled during the design of the study. In a randomized clinical trial (RCT), for instance, randomization aims to prevent third variables of interest from being unbalanced by treatment assignment, thereby reducing potential confounding. In population-based studies or clinical settings where randomization is not feasible or ethical, confounding can be mitigated through multivariable adjustment in regression models or alternative modern approaches to causal inference (e.g., propensity score methods).
Figure 1. The relationship between hypertension (exposure) and the risk of congestive heart failure (outcome variable) may be confounded by overweight (confounder), which is a risk factor for developing heart failure and is possibly associated with hypertension
It is necessary to distinguish the concept of a confounder, as previously explained, from the concept of effect modifier.
An effect modifier is a third variable whose presence modifies the strength of the association between the exposure of interest and the outcome. Unlike confounding, effect modifiers should not be adjusted or eliminated, but described.
In the previous example, diabetes may modify the effect of the relationship between hypertension (HTN) and congestive heart failure (CHF), as it may be different in those with and without diabetes. From an analytical point of view, effect modification can be detected by presenting results that are stratified by the level of the effect modifier variable (e.g., hypertension × diabetes) or by including an interaction term in the regression model. This is achieved by including the product of the effect modifier and the main exposure variable (in this example, HT x diabetes), which will have a statistically significant p – value. (Figure 2)
Figure 2. Diabetes can act as an effect modifier in the relationship between hypertension and congestive heart failure; if we stratify it and there are differences between individuals with and without diabetes, we are dealing with an effect modifier of this relationship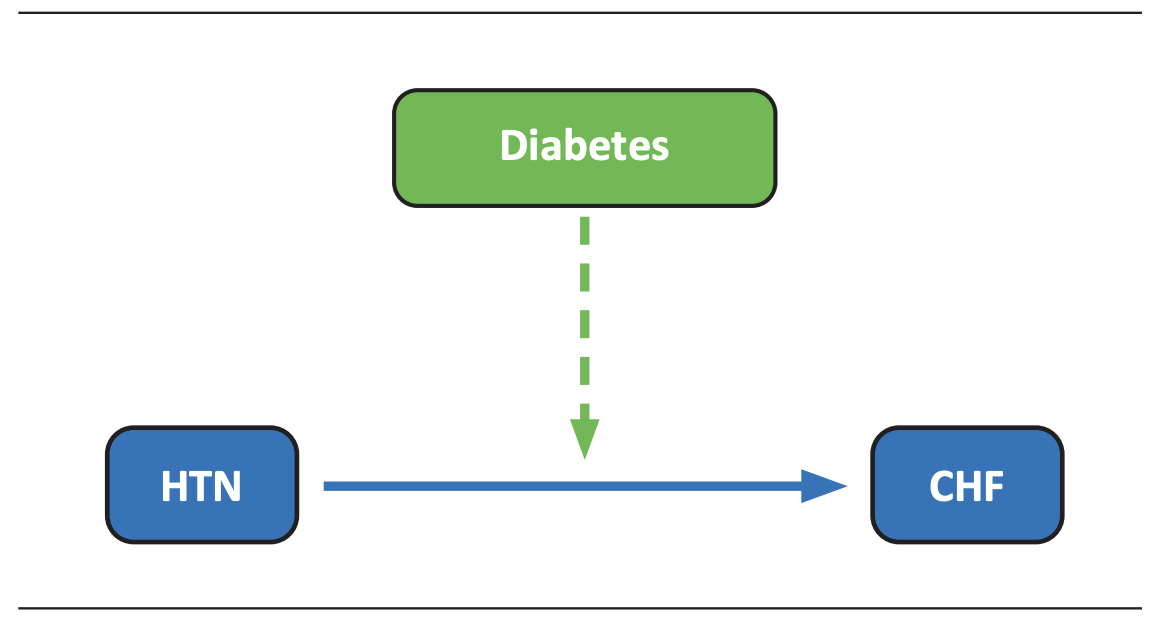
This can be exemplified as follows: Univariate analysis of the relationship between hypertension and the risk of congestive heart failure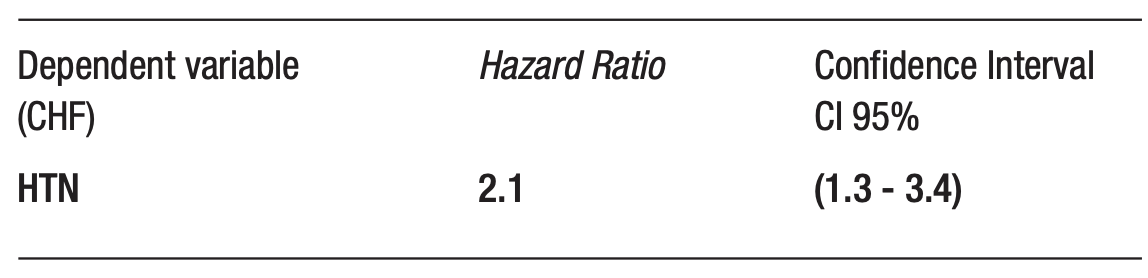
We include the overweight variable (univariate analysis
The relationship between hypertension and the risk of congestive heart failure is altered by to the presence of a second variable (overweight). The hazard ratio of the univariate relationship is attenuated when adjusting for overweight (2.1 to 1.2), and the confidence interval is less than 1, which is not statistically significant). Therefore, overweight is a confounder of the relationship between hypertension and congestive heart failure.
If we stratify by the presence or absence of diabetes: Patients with diabetes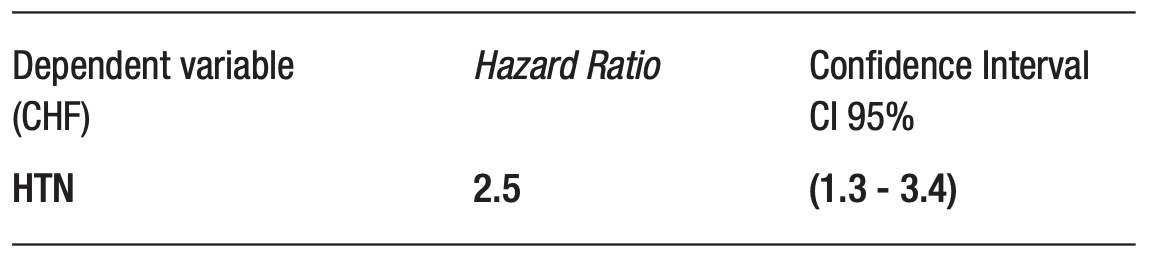
Patients without diabetes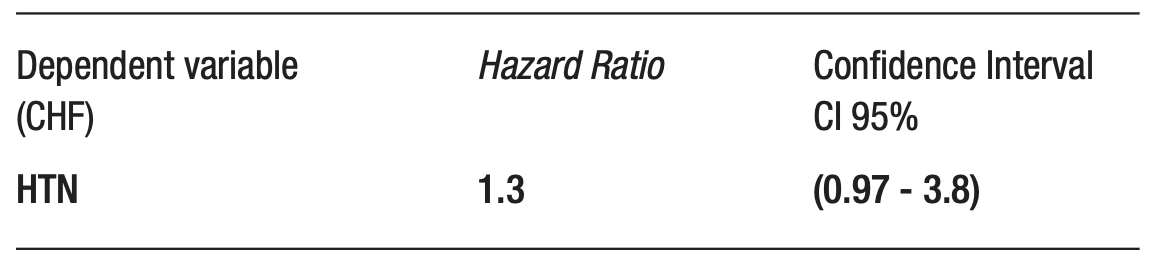
As we can see, the relationship between hypertension and congestive heart failure differs depending on whether we stratify by the presence or absence of diabetes (effect modifier); we can also include the product of the interaction of Diabetes × Hypertension in the multivariable model of heart failure.
The concept of a confounder is key in observational studies in which the aim is to assess causality, since the baseline characteristics of the participants are not balanced between groups (i.e., not randomized), and must be adjusted for.
In observational studies, confounding is a source of bias that must be controlled through design or analysis, whereas effect modification represents real heterogeneity of effect between subgroups and must be described. Distinguishing confounding factors from effect modification is a prerequisite for proper causal interpretation.
Intellectual property. The authors declare that the data and tables in this article are original and were carried out at their institutions.
Funding. The authors declare that there were no external sources of funding.
Conflict of interest. The authors declare that they have no conflicts of interest in relation to this article.
Copyright
© 2025 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Pizarro R y Barbagelata L. Confoun- ders and Effect Modifiers. Acta Gastroenterol Latinoam. 2025;55(4):273-275. https://doi.org/10.52787/agl.v55i4.560
Bibliografy
Bellavia A, Murphy SA. Confounders, Effect Modifiers, and Mediators. Circulation 2025.
Lee H et al. AGReMA statement. JAMA 2021.
Jager KJ et al. Confounding: What it is and how to deal with it. Kidney Int 2008.
Kiriakou DN, Lewis DJ. Confounding by indication. JAMA 2016.
Desai RJ, Franklin JM. Approaches for confounding adjustment. BMJ 2019.
Correspondence: Leandro Barbagelata
Email: leandro.barbagelata@hospitalitaliano.org.ar
Acta Gastroenterol Latinoam 2025;55(4):273-275

