Nicolás Lavorato ID· Alejandro Moreira Grecco ID· Tomás Flores ID· Rodrigo Morales ID· Gonzalo Hugo Zapata ID· Luis Ernesto Sarotto ID
Hospital de Clínicas «José de San Martín».
Ciudad Autónoma de Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2025;55(1):53-56
Received: 01/05/2024 / Accepted: 29/01/2025 / Published online: 31/03/2025 /
https://doi.org/10.52787/agl.v55i1.412

Summary
Intestinal malrotation is a rare congenital anomaly that occurs in approximately one in 500 to 6,000 live births and is characterized by abnormal rotation of the intestine during fetal development. Intestinal malrotation in adults is rare, occurring in only 0.17% of CT scans performed in this age group. The occurrence of colon cancer in a patient with intestinal malrotation raises important difficulties and technical factors to consider when diagnosing and treating colon cancer.
Keywords. Intestinal malrotation, colorectal cancer.
Coexistencia de cáncer de colon y malrotación intestinal: un raro desafío anatómico y oncológico
Resumen
La malrotación intestinal es una anomalía congénita poco común que ocurre en aproximadamente uno de cada 500 a 6000 nacidos vivos y se caracteriza por la rotación anormal del intestino durante el desarrollo fetal. La malrotación intestinal en adultos es una afección rara, presente en solo el 0,17% de las tomografías realizadas en este rango etario. La aparición de cáncer de colon en un paciente con malrotación intestinal plantea importantes dificultades y factores técnicos a considerar a la hora de diagnosticar y tratar la enfermedad.
Palabras claves. Malrotación intestinal, cáncer colorrectal.
Abreviatures
GIM: Intestinal malrotation.
CT: Computed tomography.
SMA: Superior mesenteric artery.
ICG: Indocyanine green.
Introduction
Intestinal malrotation (IM) is a rare congenital anomaly, estimated to occur in approximately one in 500 to 6,000 newborns, characterized by abnormal rotation of the intestine during fetal development. Most patients present with symptoms within the first month of life, although some may remain asymptomatic into adulthood. The abnormal position of the bowel often obscures the diagnosis of common diseases1 and presents unique challenges in the diagnosis and treatment of gastrointestinal disorders.
Different degrees of abnormal malrotation have been described based on computed tomography (CT) findings, such us duodenal partial rotation, duodenal nonrotation, and duodenal malrotation. Most cases present with partial duodenal rotation and jejunum located in the right abdomen. An ectopic cecum is found in a small percentage of cases.2
Concomitant malrotation and colon cancer is extremely rare. We report a case of open right hemicolectomy for colon cancer in a patient with intestinal malrotation, highlighting the anatomic landmarks considered during the preoperative workup and surgery. The presence of intestinal malrotation indicates certain anatomic peculiarities that make surgery more challenging.
Right colonic localization is more frequent in patients with colon cancer and intestinal malrotation. Surgery for resection of right colon cancers with intestinal malrotation has been successfully performed, aided by accurate preoperative imaging for delineation of vascular anatomy. In the present case, CT angiography was the key to discovering an embryologic disposition of the superior mesenteric artery (SMA) with strikingly short colic branches. The presence of abnormal anatomy and altered vascular orientation presents a challenge for resection with adequate nodal clearance.
Case
A 64-year-old woman with a medical history suggestive of iron deficiency anemia was referred after video colonoscopy reveled an adenocarcinoma of the right colon. CT staging revealed an intestinal malrotation, characterized by an ectopic cecum located on the left with the entire small bowel on the right and the colon on the left. In addition, there was a mass in the right colon. Figure 1.
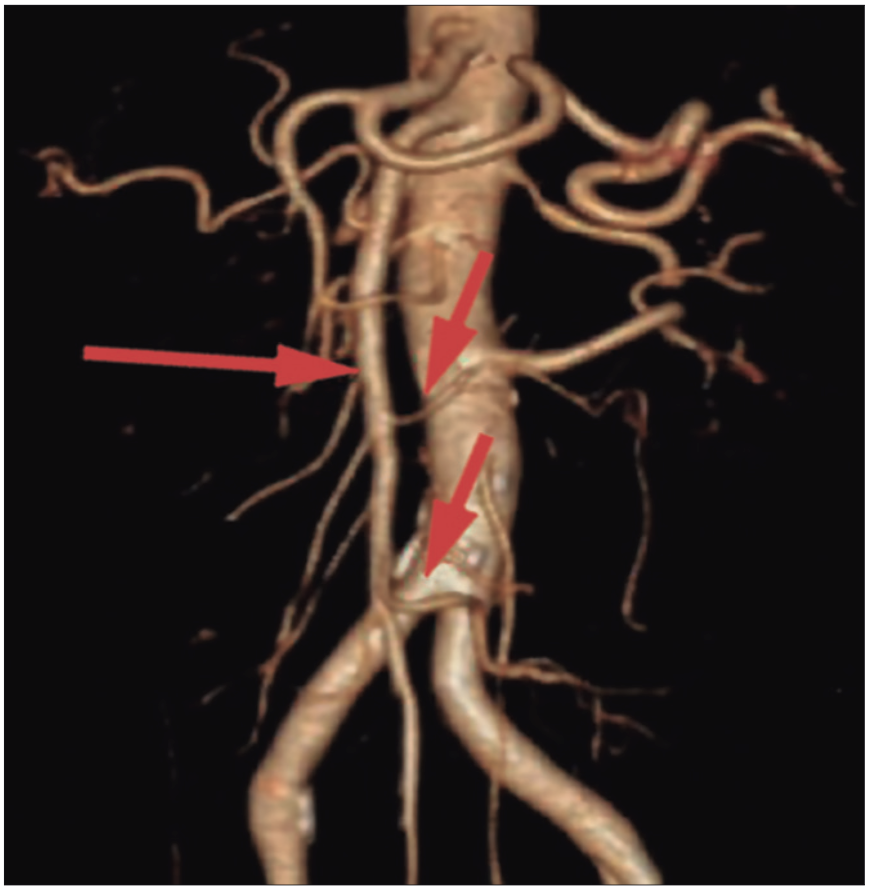
On CT angiography, the superior mesenteric artery is located to the right of the superior mesenteric vein. The right colic vessels arise directly from the superior mesenteric artery without a distinct ileocolic vessel, resembling a fetal anatomy. The left colon is supplied by the inferior mesenteric artery. Figure 2.
Figure 1. Computed tomography showing intestinal malrotation and right-sided colon cancer. Note the duodenum and small intestine to the right of the midline, the cecum to the left of the midline with a tumor. There is an abnormal disposition of the mesenteric vessels with the superior mesenteric vein anterior and to the left of the superior mesenteric artery. Red arrow: superior mesenteric artery, Blue arrow: superior mesenteric vein, yellow arrow: right colonic tumor
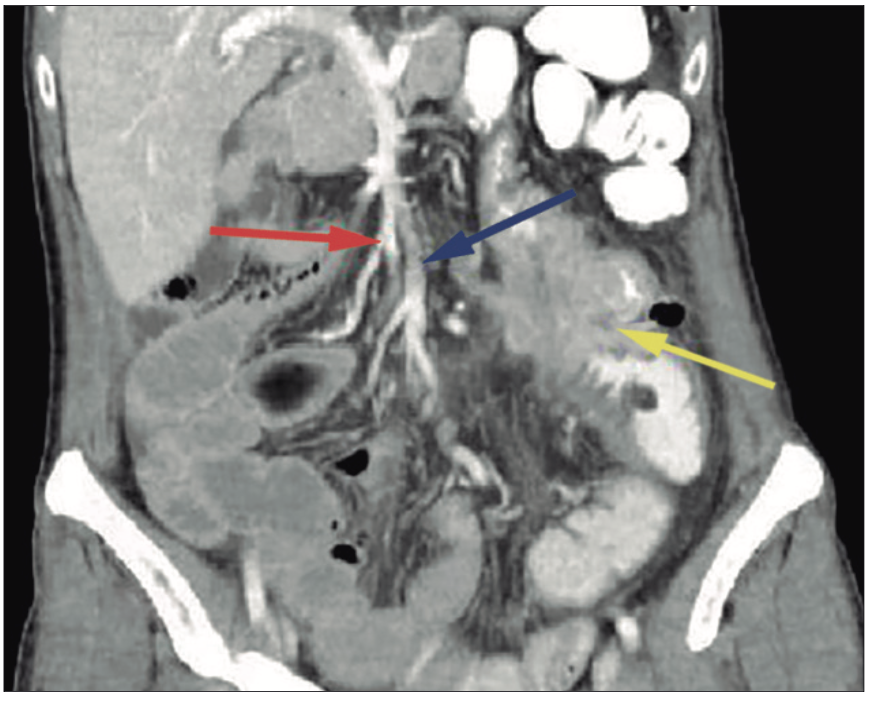
Figure 2. CT angiography of intestinal malrotation showing a superior mesenteric artery with embryonic anatomy. There is a superior mesenteric axis from which small intestinal arteries arise on the right and the right colic vessels on the left. The terminal branch irrigates the small bowel, in contrast to the anatomy of a patient with normal rotation where the terminal branch is the ileocolic artery. Long arrow: superior mesenteric artery. Short arrows: middle colic and ileocolic arteries
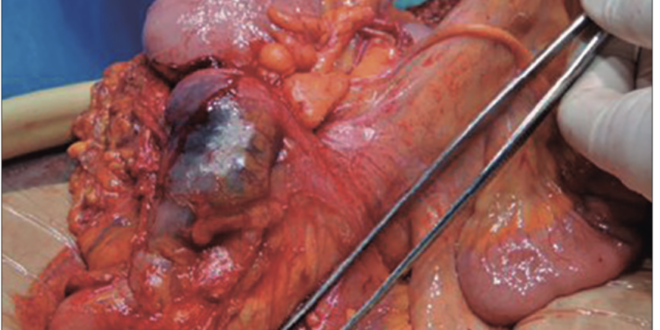
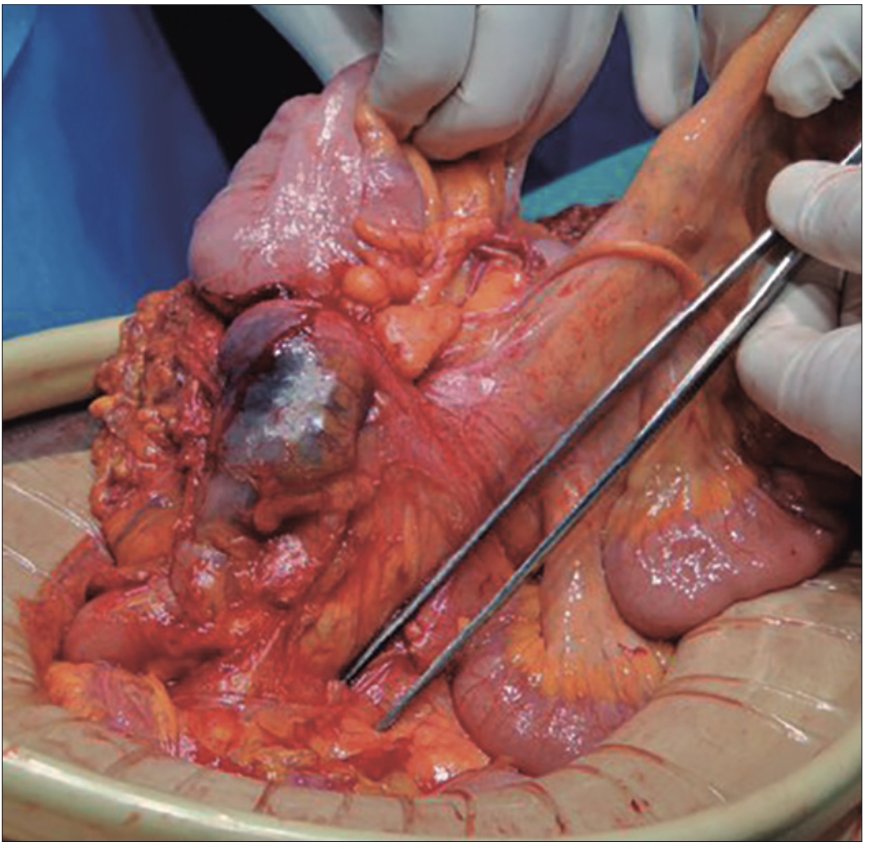
We performed an open right colectomy and found incomplete intestinal rotation with partial rotation of the duodenum, the entire jejunum to the right, and the cecum to the left of the midline. Additionally, there was a complete absence of colonic coalescence with the retroperitoneum, along with the presence of a 7 cm mass in the right colon and absence of the transverse colon. The absence of a terminal ileocolic branch, coupled with the short length of the right colic vessels, contributed to a shortened mesentery for the right colon. Figure 3. In addition, we performed intraoperative indocyanine green (ICG) angiography to assess the sufficiency of the bowel perfusion.
Figure 3. Right hemicolectomy with intestinal malrotation. The superior mesenteric pedicle is demonstrated with a short right mesocolon lateral to it. The forceps demonstrate the axis of the superior mesenteric artery
In the days following the surgery, the patient evolved favorably, with adequate intestinal transit, without complications. Therefore, she was discharged on the sixth postoperative day.
The pathology report revealed a moderately differentiated adenocarcinoma involving the colonic serosa (T4) with vasculolymphatic embolization, 11 negative lymph node with a tumor deposit 2 cm in diameter.
Discussion
Adults intestinal malrotation is a rare condition, found in only 0.17% of adults screening CT scans.3
The Japanese review of intestinal malrotation published by Nakatani identified only 49 cases of malrotation and colorectal cancer in Japan.4 A review by Taha et al. identified very few cases of malrotation associated with colorectal cancer in the literature.5 Even rarer is the presentation, as in our case, with a tumor without prior symptoms of intestinal obstruction.
Surgery should be performed with a detailed preoperative plan to avoid injury to the superior mesenteric artery and to achieve adequate lymph node dissection. The short mesentery and the atypical branching pattern of the vessels may lead to technical errors when approached as in a routine colectomy. This short mesentery presents two challenges to the surgeon. The first is to perform vascular ligation of the colic vessels without compromising the small intestine while ensuring adequate lymph node dissection. If diagnosed preoperatively, 3D CT angiography should be used to reveal the vascular anatomic anomalies for safe performance of laparoscopic surgery. In our case, CT angiography was used to diagnose the abnormal disposition of the mesenteric vessels and the short colic branches and to plan the ligation of the colic vessels. In this case, where the vascular distribution is not normal, the addition of a ICG angiography aided in intraoperative decision making.
Conclusion
The occurrence of colon cancer in a patient with intestinal malrotation poses significant difficulties and technical factors to be considered in the diagnosis and treatment of colon cancer.
Consent for publication. Written informed consent was obtained from the patient or the patient’s parent, guardian, or family member for publication of the data and/or clinical images for the benefit of science. A copy of the consent form is available to the editors of this journal.
Intellectual Property. The authors declare that the data and figures in the manuscript are original and were performed at their respective institutions.
Funding. The authors declare that there were no external sources of funding.
Conflicts of interest. The authors declare that they have no competing interests related to this article.
Copyright

© 2025 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Lavorato N, Moreira Grecco A, Flores T et al. Coexisting Colon Cancer and Intestinal Malrotation: A Rare Anatomic and Oncologic Challenge. Acta Gastroenterol Latinoam. 2025;55(1):53-56. https://doi.org/10.52787/agl.v55i1.412
References
- Norris JM, Owusu D, Abdullah AA, Rajaratnam K. Subhepatic caecal tumour in an adult with intestinal malrotation. Case Reports. 2014 Oct 29;2014.
- Xiong Z, Shen Y, Morelli JN, Li Z, Hu X, Hu D. CT facilitates improved diagnosis of adult intestinal malrotation: a 7-year retrospective study based on 332 cases. Insights Imaging. 2021 Dec 30;12(1):58.
- Perez AA, Pickhardt PJ. Intestinal malrotation in adults: prevalence and findings based on CT colonography. Abdominal Radiology. 2021 Jul 9;46(7):3002-10.
- Nakatani K, Tokuhara K, Sakaguchi T, Yoshioka K, Kon M. Laparoscopic surgery for colon cancer with intestinal malrotation in adults: Two case reports and review of literatures in Japan. Int J Surg Case Rep. 2017;38:86-90.
- Taha A, Aniukstyte L, Enodien B, Staartjes V, Taha-Mehlitz S. Intestinal Malrotation Associated With Invagination of the Distal Ileum and Cancer of the Cecum: A Case Report and Literature Review. Cureus. 2021 Mar 1;13 (3).
Acta Gastroenterol Latinoam 2025;55(1):53-56
