Nitin Kumar Bansal, Nilanjan Panda, Alagammai PL, Mohan Narsimhan, Ramesh Ardhanari
Meenakshi Mission Hospital & Research Centre.
Lake Area, Melur Road, near Mattuthavani Bus Stand, Madurai, Tamil Nadu 625107, India.
Acta Gastroenterol Latinoam 2017;47(4):252-258
Recibido: 22/10/2016 / Aprobado: 13/09/2017 / Publicado en www.actagastro.org el 18/12/2017

Summary
Objective. Asses role of EUS in patients with intermediate and high risk of CBD stone before ERCP. Design. A retrospective analysis over one-year period of patients with intermediate and high probability of CBD stones based on ASGE guidelines 2010 that underwent EUS +/- ERCP. All these patients underwent EUS first, followed by ERCP if stones/ sludge were detected. ERCP was deferred if EUS was normal. These patients were followed up for six months. Results. EUS showed CBD stone/ sludge in 112 out of 170 patients (65.9%). All these 112 patients underwent ERCP in the same session. All patients had stone/ sludge in ERCP thus giving EUS a specificity of 100%. By this EUS first strategy, we were able to avoid ERCP for 58 patients (34.1%), p value < 0.001. Among those in high risk category (where we had excluded cholangitis), ERCP was avoided in 35% of patients (p < 0.026). Cost analysis showed EUS first strategy to be 6.11% cheaper than direct ERCP strategy in this group. If we take only high-risk patients where ERCP first is the standard guideline, the cost comes down by 7%. If we also consider costs of possible ERCP complications in EUS negative patients (n = 58) who avoided ERCP, the predicted cost advantage will be more. Conclusion. EUS is a safe and accurate modality to detect CBD stones. A EUS first strategy will help to filter patients for therapeutic ERCP. This avoids unnecessary ERCP related complications and cost.
Key words. EUS, ERCP, cholelithiasis, choledocholithiasis, biliary pancreatitis.
Beneficios de la ecoendoscopía. Primera estrategia en pacientes con riesgo intermedio y alto de coledocolitiasis
Resumen
Objetivo. Analizar el papel de la ecoendoscopía (EE) en pacientes con riesgo intermedio y alto de litiasis en la vía biliar, antes de realizar la colangiopancreatografía retrógrada endoscópica (CPRE). Diseño. Análisis retrospectivo en un período de un año de pacientes con probabilidad intermedia y alta de cálculos en la vía biliar (CVB), basado en las guías de la ASGE 2010, que se sometieron a EE +/- CPRE. Todos los pacientes fueron sometidos primero a EE, seguidos por CPRE si se detectaron litos y/o barro biliar. La CPRE no se realizó cuando la EE era normal. Se realizó seguimiento a los pacientes durante seis meses. Resultados. La EE mostró CVB en 112 de 170 pacientes (65,9%). Los 112 pacientes fueron sometidos a CPRE en la misma sesión. Todos tenían litos/ barro en la CPRE, por lo que la EE tuvo una sensibilidad del 100%. Por esta primera estrategia de la EE, pudimos evitar la CPRE en 58 pacientes (34,1%, p < 0,001). Entre los que estaban en la categoría de alto riesgo (se había excluido la colangitis), la CPRE se evitó en el 35% de los pacientes (p < 0,026). El análisis de costos mostró que la primera estrategia de EE era 6,11% más barata que la estrategia de CPRE directa en este grupo. Si solo tomamos pacientes de alto riesgo en los que CPRE es la guía estándar, el costo disminuyó en un 7%. Si también consideramos los costos de las posibles complicaciones de la CPRE en pacientes EE negativos (n = 58) que evitaron la CPRE, la ventaja pronosticada del costo sería mayor. Conclusión. EE es un método seguro y preciso para detectar CBV. Una primera estrategia de EE ayudará a filtrar a los pacientes para CPRE terapéutica, y evitar complicaciones y costos innecesarios relacionados con la CPRE.
Palabras claves. Ecografía, CPRE, colelitiasis, coledocolitiasis, pancreatitis biliar.
Cholelithiasis is a common condition, 10-15% of them may have coexisting choledocholithiasis1 they may be asymptomatic or present with jaundice, deranged liver functions, cholangitis or biliary pancreatitis. Diagnosing choledocholithiasis preoperatively is crucial in decision making especially in laparoscopic era. Thus, an accurate and safe method to detect common bile duct (CBD) stones is essential.
Generally clinical suspicion of a possible coexisting CBD stones gives the first clue. Initial investigations needed are the liver function tests (LFT) and ultrasounds of the abdomen which then help to risk stratify the patients. Trans abdominal ultrasonography is a cheap, widely available and noninvasive but has low sensitivity (25- 82%) and specificity (56-100%) for detection of CBD stones.1, 2 Various modalities like computer tomography (CT), magnetic resonance cholangiography (MRCP), endoscopic ultrasonography (EUS), diagnostic endoscopic retrograde cholangio-pancreatography (ERCP) and intraoperative cholangiogram/choledocoscopy are available to look for CBD stones with each having its own advantages and drawbacks. MRCP and EUS are the two preoperative reliable investigations which diagnose choledocholithiasis with sensitivity of more than 95% and specificity of more than 97%.3 ERCP is another modality with a very high accuracy where a therapy can be performed when a diagnosis of CBD stones is confirmed.4 Unfortunately ERCP is associated with high complication rate thus making it less favorable for only diagnostic purposes.5
Since its introduction in 1989, EUS has established itself as very sensitive, specific and minimally invasive procedure for the diagnosis of CBD stones with least complication rate.6 The major advantage of EUS over transabdominal ultrasonography is that ultrasound transducer is into the second part of the duodenum and interference from digestive gas or abdominal fat is avoided while viewing the biliary tree. EUS can detect small stones/ sludge and even microlithiasis making it a preferred modality for preoperative diagnosis of choledocholithiasis in patients with intermediate risk. EUS has been shown to pick up stones missed in MRCP.7 Because of high sensitivity, specificity and noninvasive nature with negligible complication rate, EUS has replaced diagnostic ERCP even in high-risk cases in some centers.8 However, standard recommendations in high risk cases still is ERCP without additional imaging. The aim of this study was to evaluate the benefits of EUS before ERCP in patients with both intermediate and high risk for choledocholithiasis.
Material and methods
A retrospective analysis of the case records of all the patients who underwent EUS +/- ERCP for suspected or diagnosed choledocholithiasis in the time period from January 2013 to June 2014 was performed.
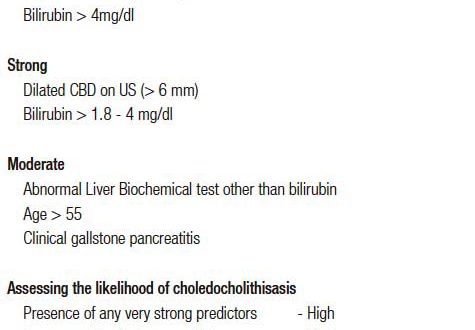
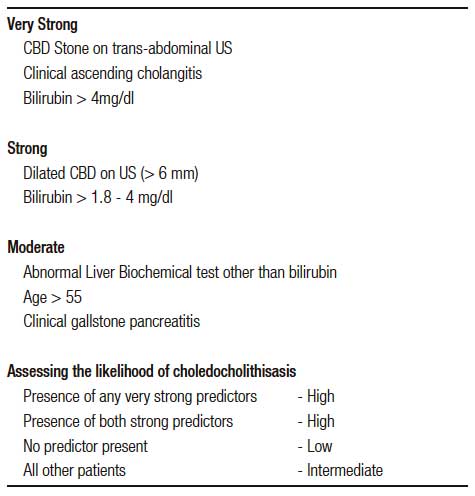
Those with cholangitis, where an emergency ERCP is indicated were excluded from the study. Those who had intermediate and high probability of having CBD stones based on ASGE guidelines 2010 were included for the study (Table 1).9
Tabla 1. Predictors of choledocholitiasis.
As per the institutional protocol, all these patients underwent EUS first, followed by ERCP if stones/ sludge were detected in EUS (Table 2). ERCP was deferred if EUS was normal and these patients were followed up for a minimum of six months. Patients without a minimum of six months follow up were excluded from the study.
All the EUS exams were performed with Pentax radial echoendoscope EG- 3630 UR (5-20 MHz, processor Hitachi-EUB-5500). A single experienced radiologist trained in endoscopy did all EUS procedures. ERCP was done by standard methods under conscious sedation by experienced gastroenterologists.
Results
A total of 170 patients were included. All of them had either a high or an intermediate probability of having CBD stones; 77 (45.3%) were male and 93 (54.7%) were female with a median age of 47.9 years (range: 18- 87) (Table 3). Sex difference was not significant.
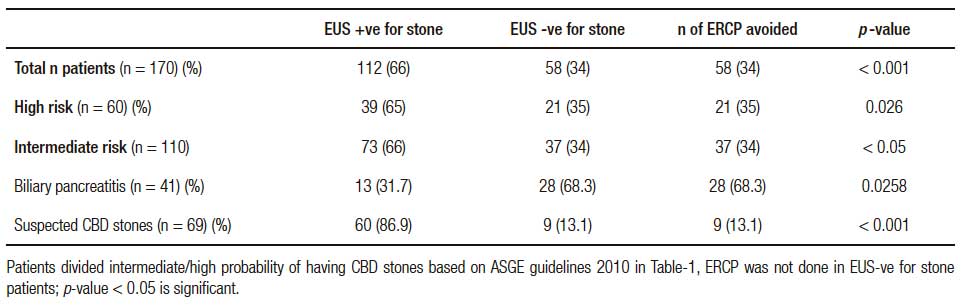
EUS was performed in all 170 patients. There were no complications related to EUS. EUS showed CBD stone/ sludge in 112 patients (65.9%). All these 112 patients underwent ERCP in the same session. Sedations were administered by anesthetists without any untoward effect. All patients had stone/sludge in ERCP thus giving EUS a sensitivity of 100% (Table 4). The rest of the 58 patients were not subjected to ERCP. They underwent cholecystectomy and were followed up for the next six months. None of them had any complications related to biliary stone during this period. Considering this, EUS has a sensitivity of 100%. By this EUS first strategy, we were able to avoid ERCP for 58 patients (34.1%), p < 0.001, which is significant. On subgroup analysis, among 41 patients with biliary pancreatitis who underwent EUS, only 13 patients required ERCP after EUS. Rest of 28 (68.3%) patients had normal EUS and so they did not require ERCP (p < 0.05). Among those in high risk category (where we had excluded cholangitis), ERCP was avoided in 35% of patients (p < 0.026). In published literature, this is around 10%. However, if we include both moderate and high-risk cases, our data is similar to published literature i.e. 10 to 60 percent, varying widely between studies.10, 11 We know many times the small stone/sludge that causes pancreatitis spontaneously pass. This may explain higher rate of EUS negative cases in our group as many cases were referred from other centers and EUS was delayed by 24 to 48 hours. However, time from onset of pancreatitis to EUS was not analyzed in this study but may be investigated in further studies. Also of note, the clinical data, laboratory data, and ultrasonography findings correctly identified 65.9% with suspected CBD stones which is similar to other studies.12
Tabla 2. Management strategy.
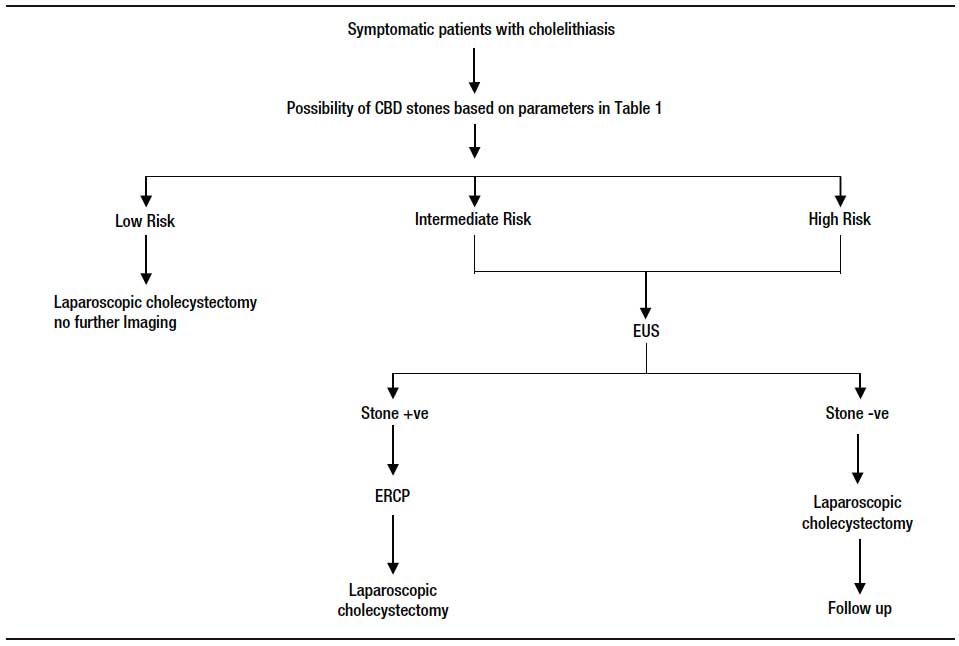
Tabla 3. Patient characteristics.
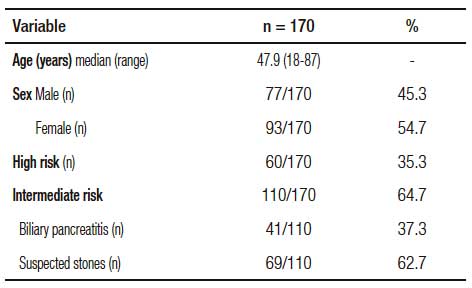
Tabla 4. EUS and ERCP: results.
Cost analysis
In our institution, we could do EUS and ERCP in the same sitting, and the cost of MRCP was similar to EUS. Hence EUS was preferred over MRCP EUS in our hospital costs Rs 7000 inclusive of cost of anesthesia and each ERCP costs Rs 25000 including admission and anesthesia cost. If all of our 170 patients had to undergo ERCP the total cost would have been Rs 42,50,000. But with our protocol 112 patients underwent EUS + ERCP and 58 patients required only EUS at the cost of Rs 35,84,000 and Rs 4,06,000 respectively (total expenditure for EUS alone and EUS+ERCP= Rs 39,90,000). We were able to save a total of Rs 2,60,000. If we look into the high-risk group only, the cost saving is Rs 105000, i.e. seven percent. If we also consider costs of possible ERCP complications in EUS negative patients (n = 58) who avoided ERCP, the predicted cost advantage will be more. However, in this study we have not looked into ERCP complications.
Discussion
In our series, we analyzed the role of EUS prior to ERCP in patients with suspected choledocholithiasis having intermediate and high probability. EUS was 100% sensitive; all those who had abnormal finding in EUS were confirmed to have the same finding in ERCP as well. EUS negative patients were followed up for six months. None of them had any biliary complications. We considered patients as true negative if they were symptom free for six months. Data from Napoleon et al, who followed up 238 patients with suspected CBD stones but with normal EUS showed that all cases of missed CBD stones were detected within a month.13
Though EUS is observer dependent, it has been shown to be very useful in the study of the extrahepatic biliary tree. The Ultrasound probe is close to the CBD making detailed imaging possible. Together with its excellent safety profile and minimally invasive nature, EUS is an excellent method to study the biliary system. Our observation stating that EUS has good sensitivity and specificity to detect CBD stones is concordant with the available literature.14-17
The main purpose of our study was to assess the benefits of EUS as a triage tool to select patients for therapeutic ERCP. By our EUS first strategy, we were able to avoid ERCP in about 1/3rd of the patients. Lee et al performed a prospective randomized study to compare EUS first vs. ERCP first in suspected choledocholithiasis18 they showed the procedure related complications are much higher in ERCP first group and by using EUS as a triage tool, diagnostic ERCP and related complications could be avoided in nearly 75% of their patients. Similarly, Ang et al. prospectively analyzed the advantages of EUS first strategy in patients with suspected choledocholithiasis with a normal trans-abdominal USG. They showed that EUS first approach could avoid ERCP in 30% of cases.19 Systematic review of randomized controlled trials by Petrov et al concluded that EUS can avoid ERCP in two-thirds of patients and application of EUS in the selection of patients for therapeutic ERCP significantly reduces the overall complication rate.20
The benefit of EUS as a triage tool is accepted in studies in low risk and intermediate risk patients.14, 21-22 In 2010 ASGE guideline, for low risk case, direct cholecystectomy is advised. In intermediate risk cases, either preoperative imaging with MRCP or EUS or intraoperative cholangiogram is advised. Those with high probability of CBD stones (high-risk group) can undergo direct ERCP with a diagnostic and therapeutic intent.23 However, ERCP is associated with a small but significant risk of morbidity and mortality, including severe complications, such as acute pancreatitis; bleeding; perforation; sepsis; and rarely, death. Though ASGE prefers direct ERCP for high-risk category, some of the authors have shown benefits with EUS first protocol in this high-risk group as well.8, 24 In our study, a subgroup analysis of patients with high risk revealed that ERCP was avoided in 35% of patients by doing EUS prior to ERCP (significant p < 0.5). We included patients with dilated CBD with abnormal LFT or CBD stone documented by transabdominal USG or those with high bilirubin (> 4 mg %) as high-risk category. We excluded cholangitis since studies have shown EUS to be unnecessarily adding to the cost in this patients.19
EUS is also recommended in patients where risk of pancreatitis and/or radiation exposure would make confirmatory testing desirable prior to ERCP. Examples of the latter include patients with gallstone pancreatitis, pregnant women, and those with other risk factors for complications from ERCP.25 EUS usually lack therapeutic options if CBD stones are detected, but it can help to avoid unnecessary ERCPs. Also, in failed ERCP cannulation, EUS guided biliary access can be attempted.26
Biliary pancreatitis, which is considered to be an intermediate risk category for the presence of CBD stones, is a definite indication of EUS/ MRCP/ intraoperative cholangiogram. CBD stones are expected to be present in 10- 50% of cases.8, 9 If residual stones are missed, this can lead to recurrent pancreatitis episodes or cholangitis. By our EUS first strategy, we found that only 1/3rd of the patients with biliary pancreatitis required ERCP. Our results are in concordance with similar studies.19, 27 A systematic review published in this context showed EUS to be noninvasive avoiding ERCP in more than 70% of cases.28
The cost effectiveness of EUS followed by ERCP had been studied by many authors. Alhayaf et al retrospectively analyzed the cost effectiveness of EUS followed by ERCP if needed in moderate and high-risk category. They documented cost savings based on the number of ERCPs avoided as well the possible post ERCP complications if those were done.29 Ang et al analyzed the cost effectiveness and found EUS based strategy to be costlier only in patients with biliary sepsis. For all other categories, there was no significant cost difference.19 With our policy of EUS first approach we were able to save a total amount of Rs 2,60,000 translating into Rs 1530 per patients (which makes EUS first strategy to be 6.11% cheaper than direct ERCP strategy). If we take only high-risk patients where ERCP first is the standard guideline, we have saved Rs 1750 per patients (i.e. 7% cheaper). If we take into account risk of development of post-ERCP pancreatitis which in recent prospective studies varied between 1 and 13.5%, the cost saving becomes much more significant. A separate study can be undertaken with larger number of patients for possible analysis of full cost benefit.
We performed all our EUS and ERCP in the same session. The issue which is often discussed when EUS and ERCP are done in the same session is sedation and its complications. Generally, the amount of sedation used is higher and so the recovery time is longer if EUS and ERCP are combined. Despite this fact, retrospective studies have shown combined EUS and ERCP to be safe with no additional sedation related or procedure related complications.30 Postponing the ERCP when it is indicated could result in interval period complications like cholangitis/pancreatitis.31, 32 In our patients, we did not have any major sedation related complications (of note, anesthetists were present in all the cases).
Despite its overall high accuracy, the role of EUS in the diagnosis of CBD stones has not been firmly established as it is relatively invasive without any therapeutic role. EUS carries small risks of sedation, bleeding, and perforation. It has the limited availability of the machine and trained staff compared to MRCP.33 Also intra-hepatic stones is more difficult to identify at EUS.34
Both radial and linear echoendoscopes are reliable for evaluation and detection of choledocholithiasis. A higher resolution of EUS (EUS 0.1 mm vs. MRCP of 1.5 mm), increase chances of detecting smaller stones and sludge. In EUS, images can be manipulated via magnification and alterations in endoscope position and US frequency in real time for better visualization. MRCP is done in a separate location, often on a separate day and is time consuming. A systematic review comparing EUS to MRCP found similar overall diagnostic performance suggesting that the choice between them should be based upon the availability of resources, experience, and costs.35
Studies found EUS before ERCP was cheaper to either MRCP before ERCP or ERCP alone in low-to-moderate–risk patients.36 EUS use for low-to-moderate–risk patients significantly reduced number of ERCP’s, but decision analysis models on the value of MRCP have not universally demonstrated a reduction in the number of ERCPs performed in patients with suspected choledocholithiasis or other pancreatobiliary diseases.37, 38
With our data showing advantage of EUS prior to ERCP in high risk patients as well, we need to conduct studies with MRCP prior to ERCP in this category. However available data has shown that MRCP use is associated with increased cost and length of stay but does not influence patient or procedural outcomes in high risk patients.39
Conclusions
In any patient with symptomatic cholelithiasis, treating surgeon should have a suspicion of coexisting choledocholithiasis based on clues given by clinical, biochemical and radiological parameters. EUS is a minimally invasive, safe and accurate modality, which can be relied upon to detect CBD stones. A EUS first strategy will help to filter patients for therapeutic ERCP. This can avoid ECRPs in a good proportion of patients including high risk group thus avoiding unnecessary ERCP related complications and cost.
References
- Hunter JG, Soper NJ. Laparoscopic management of bile duct stones. Surg Clin North Am 1992; 72: 1077-1097.
- Pickuth D, Spielmann RP. Detection of choledocholithiasis: comparison of unenhanced spiral CT, US, and ERCP. Hepatogastroenterology 2000; 47: 1514-1517.
- de Lédinghen V, Lecesne R, Raymond JM, Gense V, Amouretti M, Drouillard J, Couzigou P, Silvain C. Diagnosis of choledocholithiasis: EUS or magnetic resonance cholangiography? A prospective controlled study. Gastrointest Endosc 1999; 49: 26-31.
- Prat F, Amouyal G, Amouyal P, Pelletier G, Fritsch J, Choury AD, Buffet C, Etienne JP. Prospective controlled study of endoscopic ultrasonography and endoscopic retrograde cholangiography in patients with suspected common bile duct lithiasis. Lancet 1996; 347: 75.
- Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, Dinelli M, Minoli G, Crosta C, Comin U, Fertitta A, Prada A, Passoni GR, Testoni PA. Complications of diagnostic and therapeutic ERCP: a prospective, multicenter study. Am J Gastroenterol 2001; 96: 417-423.
- Amouyal P, Palazzo L, Amouyal G, Ponsot P, Mompoint D, Vilgrain V, Gayet B, Fléjou JF, Paolaggi JA. Endosonography: Promising method for diagnosis of extrahepatic cholestasis. Lancet 1989; 2: 1195-1198.
- Vázquez-Sequeiros E, González-Panizo Tamargo F, Boixeda- Miquel D, Milicua JM. Diagnostic accuracy and therapeutic impact of endoscopic ultrasonography in patients with intermediate suspicion of choledocholithiasis and absence of findings in magnetic resonance cholangiography. Rev Esp Enferm Dig 2011; 103: 464-471.
- Prachayakul V, Aswakul P, Bhunthumkomol P, Deesomsak M. Diagnostic yield of endoscopic ultrasonography in patients with intermediate or high likelihood of choledocholithiasis: a retrospective study from one university-based endoscopy center. BMC Gastroenterology 2014; 14: 165.
- ASGE Standards of Practice Committee: Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, Cash BD, Fisher L, Harrison ME, Fanelli RD, Fukami N, Ikenberry SO, Jain R, Khan K, Krinsky ML, Strohmeyer L, Dominitz JA (Chair). The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointest Endosc 2010; 71: 1-9.
- Erickson RA, Carlson B. The role of endoscopic retrograde cholangiopancreatography in patients with laparoscopic cholecystectomies. Gastroenterology 1995; 109: 252-263.
- Enochsson L, Lindberg B, Swahn F, Arnelo U. Intra-operative endoscopic retrograde cholangio-pancreatography (ERCP) to remove common bile duct stones during routine laparoscopic cholecystectomy does not prolong hospitalization: a 2-year experience. Surg Endosc 2004; 18: 367-371.
- Wang CH, Moh LR, Lin RC, Kuo YJ, Chang KK. Rapid diagnosis of choledocholithiasis using biochemical tests in patients undergoing laparoscopic cholecystectomy. Hepatogastroenterology 2005; 52: 1662-1665.
- Napoleon B, Dumortier J, Keriven-Souquet O, Pujol B, Ponchon T, Souquet JC. Do normal findings at biliary endoscopic ultrasonography obviate the need for endoscopic retrograde cholangiography in patients with suspicion of common bile duct stone? A prospective follow-up study of 238 patients. Endoscopy 2003; 35: 411-415.
- Kim MK, Lee JK, Bahng S, Shin JU, Lee KH, Lee TK, Lee WJ, Won J, Lim JH. Role of endoscopic ultrasonography in patients with intermediate probability of choledocholithiasis but a negative CT scan. Journal of Clinical Gastroenterology 2013, 47: 449-456.
- Meroni E, Bisagni P, Bona S, Fumagalli U, Zago M, Rosati R, Malesci A. Pre-operative endoscopic ultrasonography can optimize the management of patients undergoing laparoscopic cholecystectomy with abnormal liver function tests as the sole risk factor for choledocholithiasis: a prospective study. Dig Liver Dis 2004; 36: 73-77.
- Verma D, Kapadia A, Eisen GM, Adler DG. EUS vs MRCP for detection of choledocholithiasis. Gastrointestinal Endoscopy 2006; 64: 248-254.
- Sgouros SN, Bergele C. Endoscopic ultrasonography versus other diagnostic modalities in the diagnosis of choledocholithiasis. Digestive Diseases and Sciences 2006; 51: 2280-2286.
- Lee YT, Chan FKL, Leung WK, Chan HY, Wu JCY, Yung MY, Ng EKW, Lau JYW, Sung JJY. Comparison of EUS and ERCP in the investigation with suspected biliary obstruction caused by choledocholithiasis: a randomized study. Gastrointestinal Endoscopy 2008; 67: 660-668.
- Ang TL, Teo EK, Fock KM. Endosonography vs. endoscopic retrograde cholangiopancreatography-based strategies in the evaluation of suspected common bile duct stones in patients with normal transabdominal imaging. Aliment Pharmacol Ther 2007; 26: 1163-1170.
- Petrov MS, Savides TJ. Systematic review of endoscopic ultrasonography versus endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis. British Journal of Surgery 2009; 96: 967-974.
- Sotoudehmanesh R, Kolahdoozan S, Asgari AA, Dooghaei- Moghaddam M, Ainechi S. Role of Endoscopic Ultrasonography in Prevention of Unnecessary Endoscopic Retrograde Cholangiopancreatography. A prospective study of 150 patients. Ultrasound Med 2007; 26: 455-460.
- Polkowski M, Regula J, Tilszer A, Butruk E. Endoscopic ultrasound versus retrograde cholangiography for patients with intermediate probability of bile duct stones: a randomized trial comparing two management strategies. Endoscopy 2007; 39: 296-303.
- http://www.asge.org/uploadedFiles/Publications_and_Products/ Practice_Guidelines/PIIS0016510709025504.pdf.
- Tozzi di Angelo I, Prochazka V, Holinka M, Zapletalova J. Endosonography versus endoscopic retrograde cholangiopancreatography in diagnosing extrahepatic biliary obstruction. Biomedical Papers of the Medical Faculty of the University Palacký, Olomouc, Czechoslovakia 2011; 155: 339-346.
- Norton SA, Alderson D. Prospective comparison of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in the detection of bile duct stones. Br J Surg 1997; 84: 1366.
- http://www.asge.org/uploadedFiles/Publications_(public)/Practice_guidelines/ERCP_benign_diseases_biliary_tract.pdf
- Liu CL, Fan ST, Lo CM, Tso WK, Wong Y, Poon RT, Lam CM, Wong BC, Wong J. Comparison of early endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in the management of acute biliary pancreatitis: a prospective randomized study. Clin Gastroenterol Hepatol 2005; 3: 1238-1244.
- De Lisi S, Leandro G, Buscarini E. Endoscopic ultrasonography versus endoscopic retrograde cholangiopancreatography in acute biliary pancreatitis: a systematic review. European Journal of Gastroenterology & Hepatology 2011; 23: 367-374.
- Alhayaf N, Lalor E, Bain V, McKaigney J, Sandha GS. The clinical impact and cost implications of endoscopic ultrasound on the use of endoscopic retrograde cholangiopancreatography in a Canadian university hospital Can J Gastroenterol 2008; 22: 138-142.
- Che K, Muckova N, Olafsson S, Srikureja W. Safety of same-day endoscopic ultrasound and endoscopic retrograde cholangiopancreatography under conscious sedation. WJG 2010; 16: 3287- 3291.
- Benjaminov F, Stein A, Lichtman G, Pomeranz I, Konikoff F M. Consecutive versus separate sessions of endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) for symptomatic choledocholithiasis. Surgical Endoscopy 2013; 27: 2117-2121.
- Che K, Muckova N, Olafsson S, Srikureja W. Safety of same-day endoscopic ultrasound and endoscopic retrograde cholangiopancreatography under conscious sedation. World J Gastroenterology 2010; 16: 3287-3291.
- Barish MA, Yucel EK, Ferrucci JT. Magnetic resonance cholangiopancreatography. N Engl J Med 1999; 341: 258-264.
- Sivak MVJr. EUS for bile duct stones: How does it compare with ERCP? Gastrointest Endosc 2002; 56: S175-S177.
- Verma D, Kapadia A, Eisen GM, Adler DG. EUS vs. MRCP for detection of choledocholithiasis. Gastrointest Endosc 2006; 64: 248.
- Arguedas MR, Dupont AW, Wilcox CM. Where do ERCP, endoscopic ultrasound, magnetic resonance cholangiopancreatography and intraoperative cholangiography fit in the management of acute biliary pancreatitis? A decision analysis model. Am J Gastroenterol 2001; 96: 2892-2899.
- Meenan J, Tibble J, Prasad P, Wilkinson M. The substitution of endoscopic ultrasound for endoscopic retrograde cholangio-pancreatography: implications for service development and training. Eur J Gastroenterol Hepatol 2004; 16: 299-303.
- Sahai AV, Devonshire D, Yeoh KG, Kay C, Feldman D, Willner I, Farber J, Patel R, Tamasky PR, Cunningham JT, Trus T, Hawes RH, Cotton PB. The decision-making value of magnetic resonance cholangiopancreatography in patients seen in a referral center for suspected biliary and pancreatic disease. Am J Gastroenterol 2001; 96: 2074-2080.
- Anand G, Patel YA, Yeh Hsin-Chieh, Khashab MA, Lennon AM, Shin EJ, Canto MI, Okolo PI, Kalloo AN, Singh VK. Factors and Outcomes Associated with MRCP Use prior to ERCP in Patients at High Risk for Choledocholithiasis. Canadian Journal of Gastroenterology and Hepatology 2016: ID 5132052, 6 pages.
Correspondencia: Nilanjan Panda
p 318 b, CIT Road, Scheme 6 M, Kankurgachi, Kolkata 700054, India
Tel: +91 9 748774942 / +44 7 719551593
Correo electrónico: npanda05@aol.com
Acta Gastroenterol Latinoam 2017;47(4): 252-258
