Ignacio Maldonado Schoijet,1 Alberto A Rojas,2 Claudio Cortés,3 Cristian U Varela1
1 Departamento de Imagenología Clínica Dávila y Clínica Alemana. Universidad de los Andes y Universidad Mayor.
2 Departamento de Imagenología, Clínica Dávila.
3 Departamento de Imagenología Hospital Clínico, Clínica Alemana. Universidad de Chile.
Santiago de Chile, Chile.
Acta Gastroenterol Latinoam 2018;48(2):82-89
Recibido: 07/06/2017 / Aprobado: 15/02/2018 / Publicado en www.actagastro.org el 18/06/2018

Summary
Sister Mary Joseph’s nodule refers to a palpable nodule bulging into the umbilicus as result of a malignant cancer in the abdomen or pelvis. It is associated with multiple peritoneal metastases and usually indicates an advanced stage of disease with a poor prognosis. Most cases are metastatic adenocarcinoma malignancies. The most common primary sites are the gastrointestinal tract (Gastric, Colonic and Pancreas) that accounts for about a half of the underlying sources (52%) and gynecologic (ovarian and endometrial cancer, 28%). This article describes Sister Joseph`s nodule, with a brief overview from history to imaging features in computed tomography.
Key words. Sister Mary Joseph’s nodule, peritoneal neoplasms, neoplasm metastasis, gastrointestinal neoplasms, ovarian neoplasms.
Nódulo de la Hermana María José: de la historia a las imágenes. Una revisión de la literatura basada en casos
Resumen
El nódulo de la Hermana María José, se refiere a una masa palpable en el ombligo que se traduce en una neoplasia avanzada del abdomen o pelvis. Está asociado con la presencia de múltiples metástasis peritoneales y usualmente indica una enfermedad avanzada con mal pronóstico. La mayoría de los casos son neoplasias de tipo adenocarcinoma metastásico. Las causas más comunes son las neoplasias del tracto gastrointestinal (gástrico, colon y páncreas) y representa la mitad de los primarios (52%) y ginecológico (cáncer de ovario y endometrio, 28%). Este reporte busca describir el nódulo de la hermana María José, con una breve reseña de su historia y sus características en la tomografía computada.
Palabras claves. Nódulo de la Hermana María José, neoplasias peritoneales, metástasis, neoplasias gastrointestinales, neoplasias ováricas.
Sister Mary Joseph’s nodule (SMJN) is a palpable periumbilical cutaneous lesion indicative of an underlying advanced intraabdominal neoplastic disease and its presence implies a poor prognosis.1, 2 This review aims to describe the SMJN sign, focusing in its history, clinical and imaging features of multidetector computed tomography (MDCT) images, through cases.
History
The name, was originally coined by Sir Hamilton Bailey, an English surgeon and the first to mention it in its book “Demonstrations of Physical Signs in Clinical Surgery”, published in 1949, honoring the Sister Mary Joseph (1856-1939) (Figure 1), who was superintendent nurse and Dr. William Mayo most frequent first assistant, at the St. Mary’s Hospital (now Mayo Clinic) of Rochester, Minnesota.
The Sister Mary Joseph, was the first person who observed that the patients with advanced abdominal-pelvic malignancies, frequently presented a periumbilical palpable nodule.3, 4 Until now, over 400 cases has being published.5
Figure 1. Julia Dempsey (Sister Mary Joseph) (1856-1939). Born in Salamanca, New York, child of Irish immigrants, Julia Dempsey joins in 1878 the “Our Lady of Lourdes” congregation in Rochester, Minnesota, becomes a nun and adopts the name of Sister Mary Joseph. In 1889 ends the construction of the Saint Mary’s hospital, in Rochester, that latter would become the Mayo Clinic. The close relation between its congregation and the St. Mary’s hospital allows the Sister Mary Joseph to start working as a nurse in 1889 and just 6 weeks later is entitled as chief of the nursing department. A year later she becomes first surgical assistant of the Dr. William J. Mayo. Due its exceptional management capacities, 3 years later, she became superintendent of the whole hospital. At the hospital, the Mayo’s brothers soon adopted the last advances in the fields of anesthesia, asepsis/antisepsis and hemostasis; this allowed them to improve the abdominal surgical technic. In acknowledgment of the Sister Mary Joseph achievements and qualities, the Mayo brothers involved her in their surgical practice; she was in charge of the patient preparation and even started the surgery and closed the incision. In a short time, she noticed the relation between the presence of the periumbilical nodule and the advanced intraabdominal malignancy, even allowing her to “select” the patients that could be good surgery candidates with full support of the Mayo brothers. Recently, the original Saint Mary’s hospital building has been renamed as Joseph’s Hospital in her honor. http://www.historiadelamedicina.org/mariajose.html, https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101420097-img. A) Portrait of the Sister Mary Joseph; B) Drawing of the Sister Mary Joseph, noticing the nodule; C) Picture of the original dependencies of the Saint Mary’s Hospital, now Mayo Clinic. Source: Pictures from the History of Medicine (NLM). Bethesda, MD: U.S. National Library of Medicine.

Clinical features
This nodule refers to a non-sensible palpable, periumbilical nodule bulge which color varies from violaceous to reddish brown that may appear as vascular structure. Occasionally skin ulcerations or fissures with even hematic, serous or purulent discharge can be observed. The lesion diameter rarely exceeds 5 centimeters, even so, it can be larger and simulate an umbilical hernia (Figures 2, 3, 4, 5 and 7).6
The SMJN represents 1-3% of the secondary locations of the gastrointestinal malignancies.7 Despite the majority of the primary lesions that can be identified with imaging studies, in a third of the cases (15-30%) the primary lesion remains unidentified even through tissue samples (molecular biology and immunohistochemistry).8
The most frequent malignancy metastases are gastrointestinal adenocarcinomas (gastric, colon and pancreas) and gynecological (ovary and endometrium), with a 52% and 28% respectively. Gastrointestinal malignancies are, as group, the most frequent neoplasms. Gastric origin can be found as cause of the 25% of the SMJN, followed by colorectal (10%) and pancreas (7%). The types of this tumors are 75% adenocarcinomas, followed by carcinoids and undifferentiated tumors.5
Gynecological origin like epithelial ovary neoplasm and especially, the papillary cystadenocarcinoma that just by itself is the first cause of the SMJN in this group (34%).1, 9
Figure 2. Man 56 years old, advanced gastric neoplasm. A) Picture of the umbilical lesion; B) Contrast enhanced MDCT axial slice, in portal-venous phase: Large neoplastic lesion that bulge the anterior wall of the gastric wall (arrow head) with transmural involvement with non-defined borders, that invades the omentum [black asterisk (*)]; ascites [white asterisk (*)]; metastatic umbilical nodule (SMJN)(arrow).
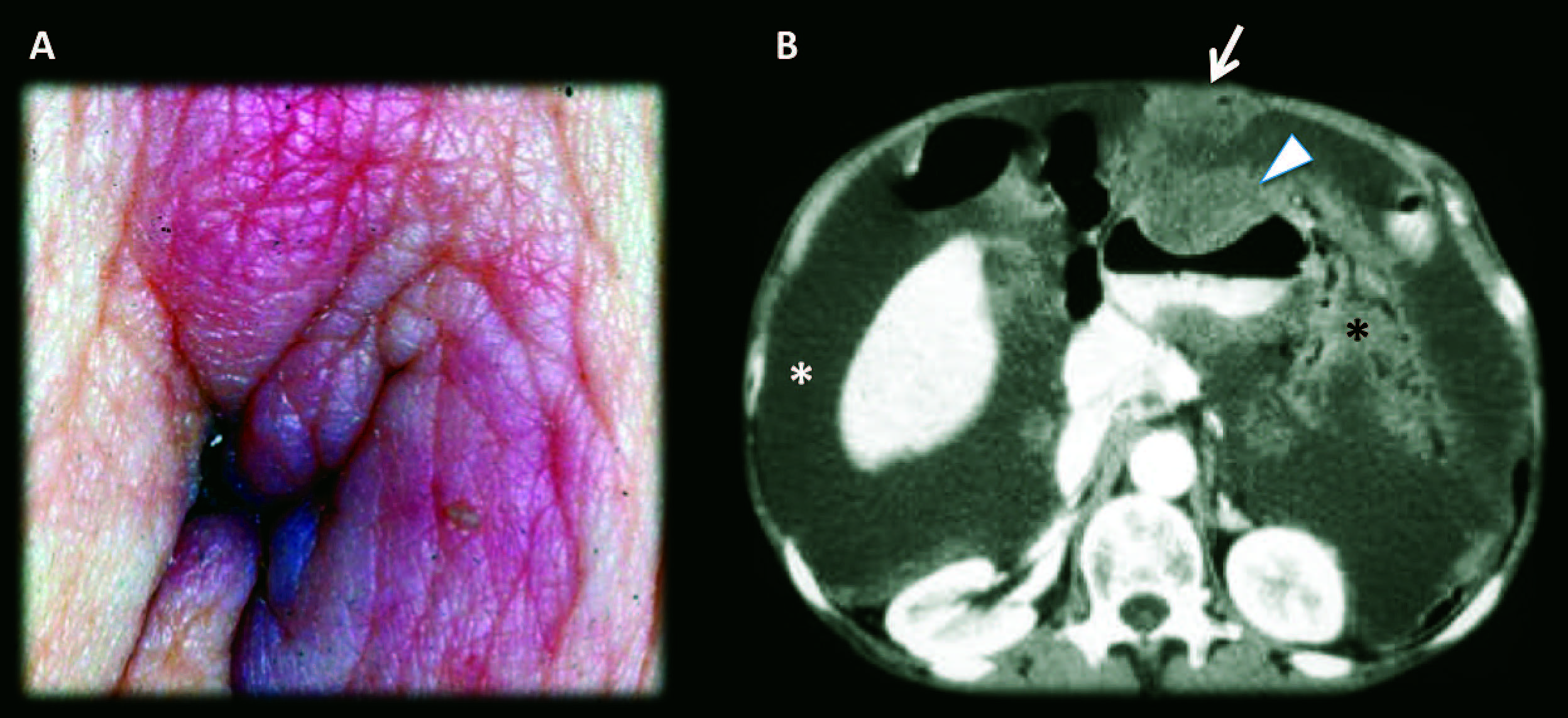
Figure 3. Man 45 years old, recurrence of surgically treated gastric neoplasm. A) Picture of the umbilical lesion; B) Contrast enhanced MDCT axial slices, in portal-venous phase: Extensive gastric neoplasm recurrence with omental involvement (omental cake) (*); Diffuse nodular peritoneal thickening and ascites (arrow head), suggests peritoneal carcinomatousis; metastatic umbilical nodule (SMJN) (arrow).
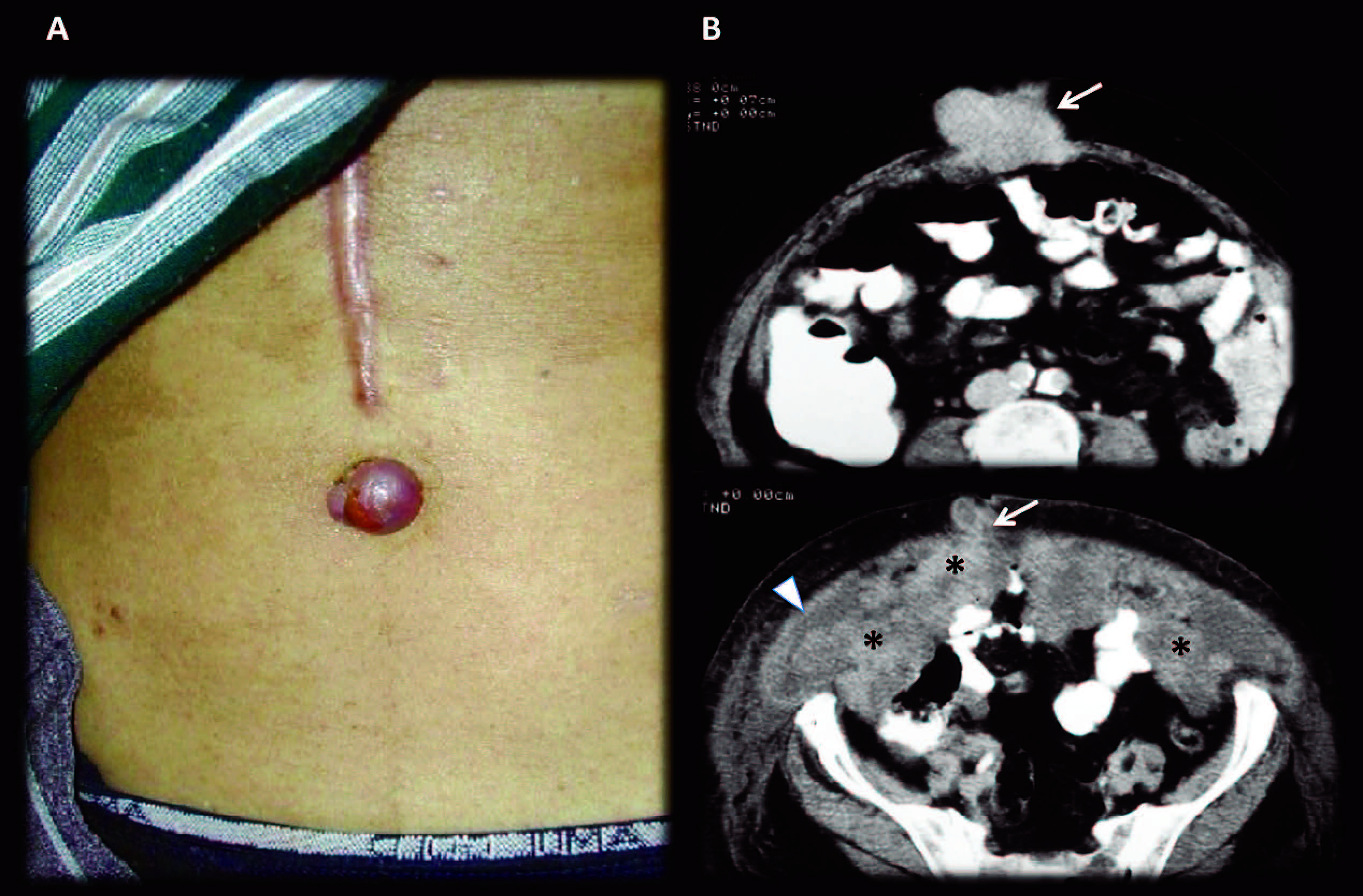
Figure 4. Man 48 years old, advanced pancreatic cancer in palliative care. Contrast enhanced MDCT axial slices, in portal-venous phase: Images shows hipovascular liver metastasis and an extensive infiltrative retroperitoneal (*), vascular and peritoneal involvement. A SMJN can be appreciated in the umbilical area (E and F). Clinicians thought that they were leading with a non-complicated umbilical hernia. Left-sided portal hypertension syndrome consists in gastric and esophagus varices with patent portal vein and extensive splenic vein thrombosis secondary tumoral invasion and replacement of splenic vein (arrows). The peritoneal involvement denotes a small amount of loculated ascites and a slightly thickening of the peritoneum with some small nodular areas (arrow head). In this exceptional case, the omentum does not appear to have macroscopic involvement.
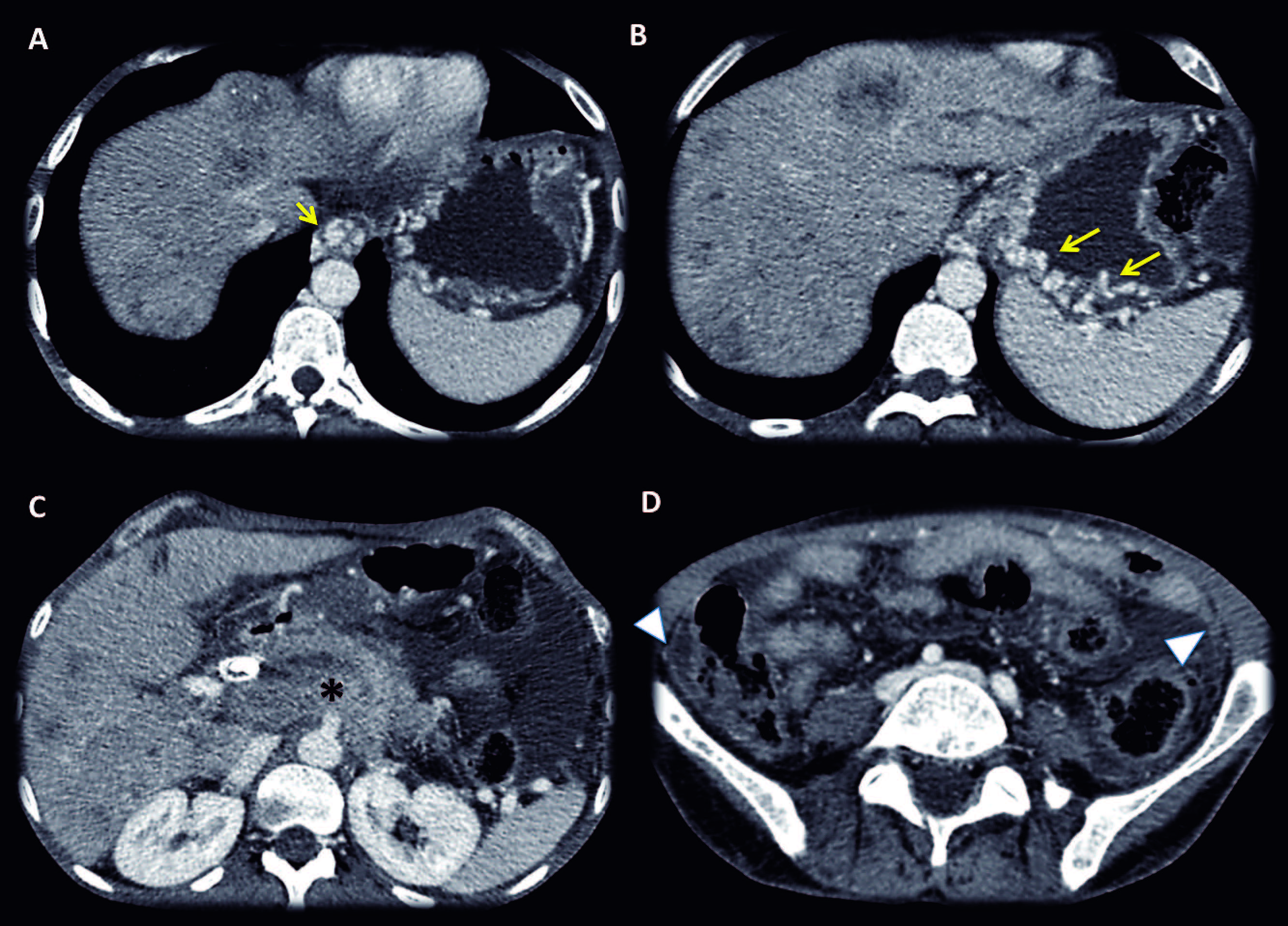
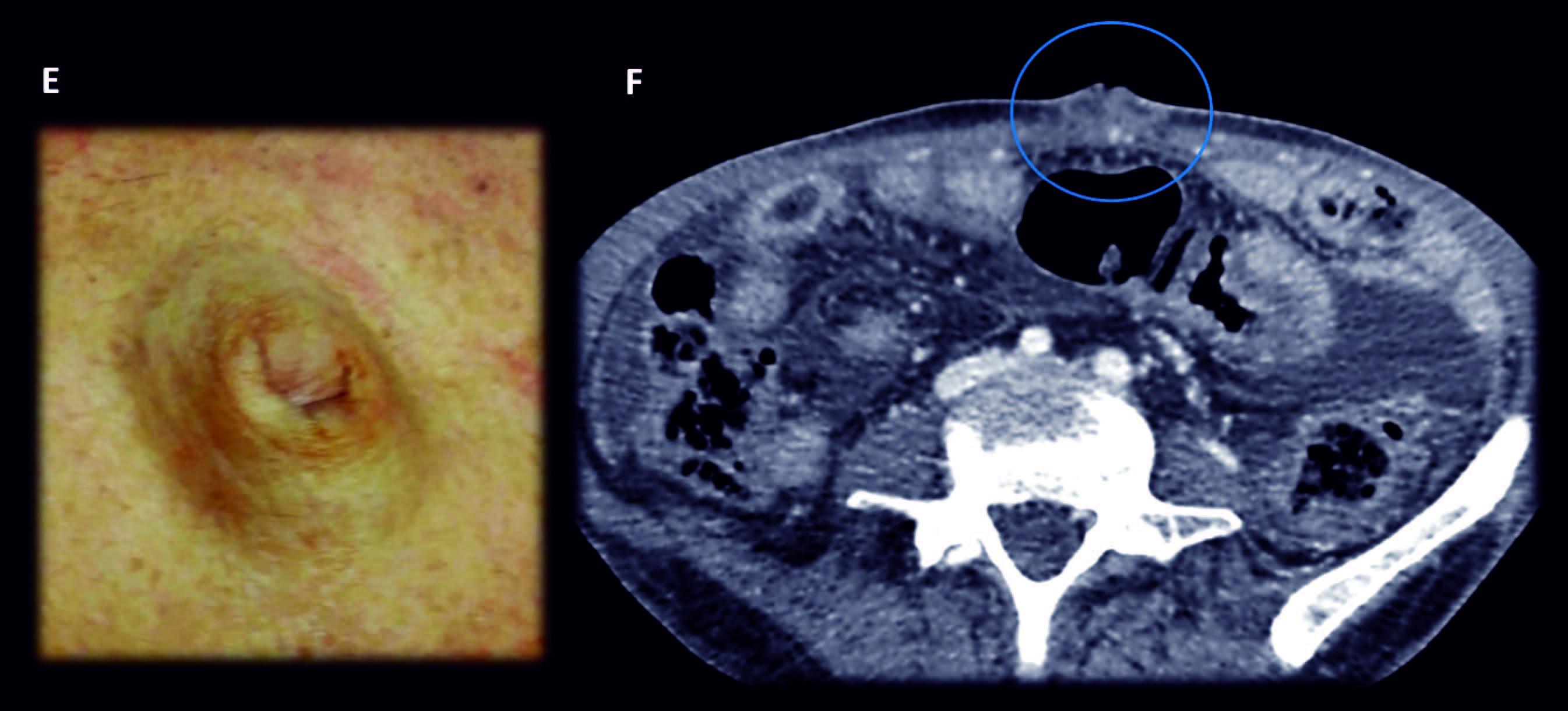
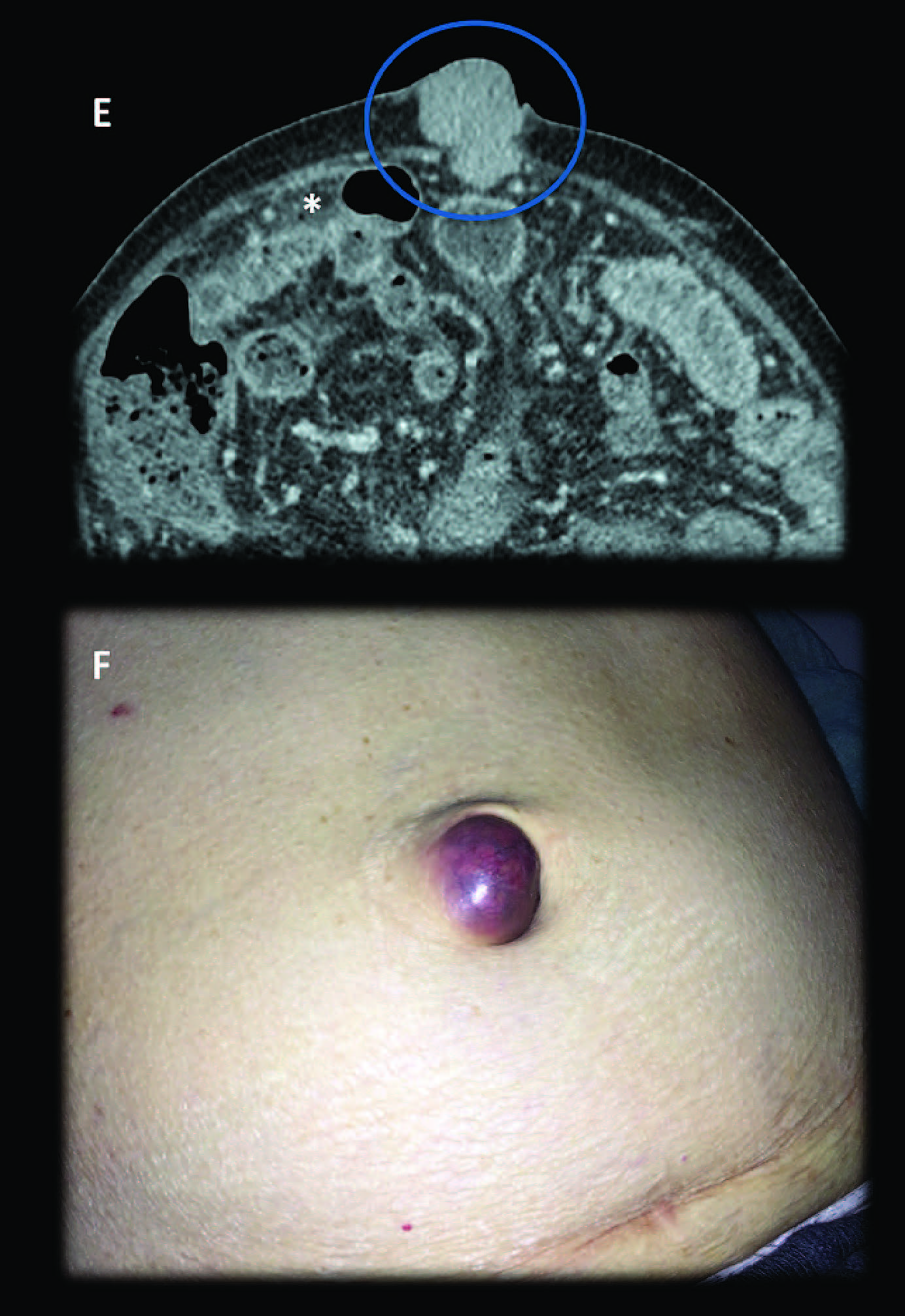
Figure 5. Man 50 years old, advanced gastric cancer in palliative care. Contrast enhanced MDCT axial slices, in portal-venous phase: (A, B, C) Huge Gastric neoplastic mass with transmural involvement with non-defined borders that invades the omentum [white asterisk (*)], hepatoduodenal and gastrohepatic ligaments [black asterisk (*)]; hipovascular liver metastasis (yellow arrows). (D, E) Metastatic umbilical nodule SMJN (volume renderings, images, blue arrow and circle).
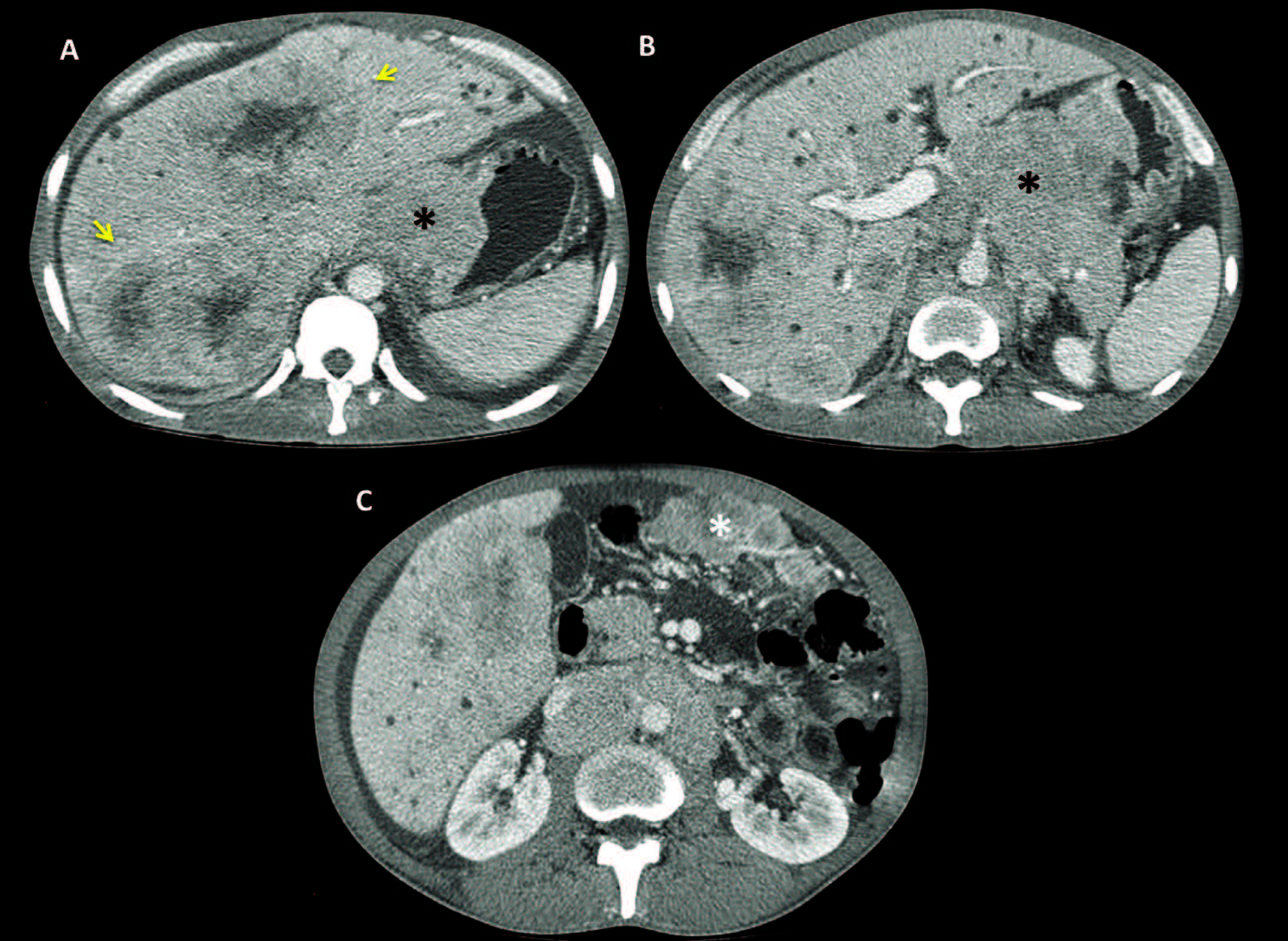
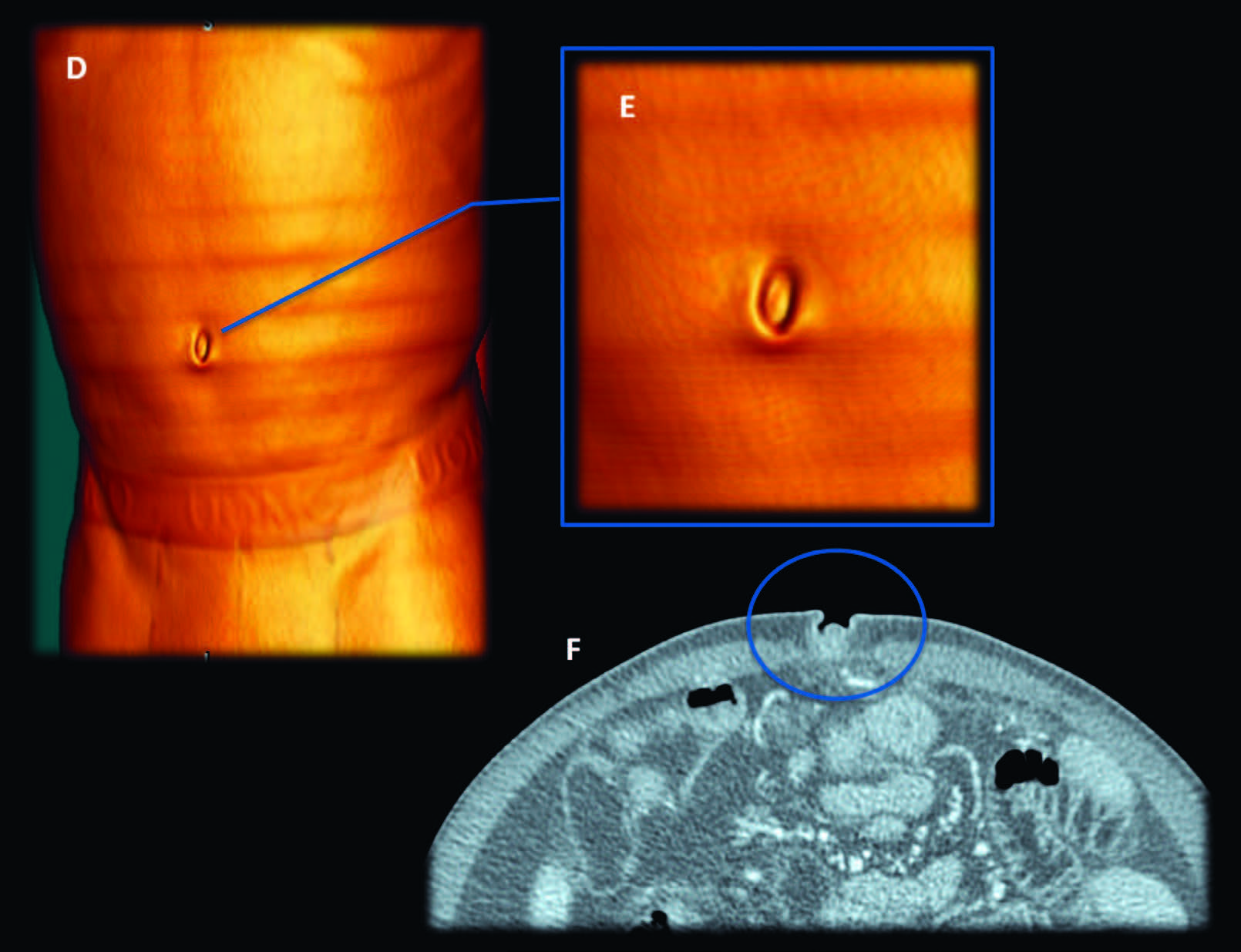
Figure 7. Female 81 years old, advanced cirrhosis. Contrast enhanced MDCT axial slices with arterial and portal-venous phase: Images shows a dysmorfic liver with severe portal hypertension and two hepatic lesions in the right lobe with early arterial enhancement with classical washout in portal venous phase, findings consistent with hepatocarcinomas (HCC). Tiny supramesocolic omental nodules (*) and peritoneal pseudonodular thickening that shows enhancement (arrows), findings that represents the peritoneal involvement. Small implant in the hepatic serosal surface in the right lobe (arrow).
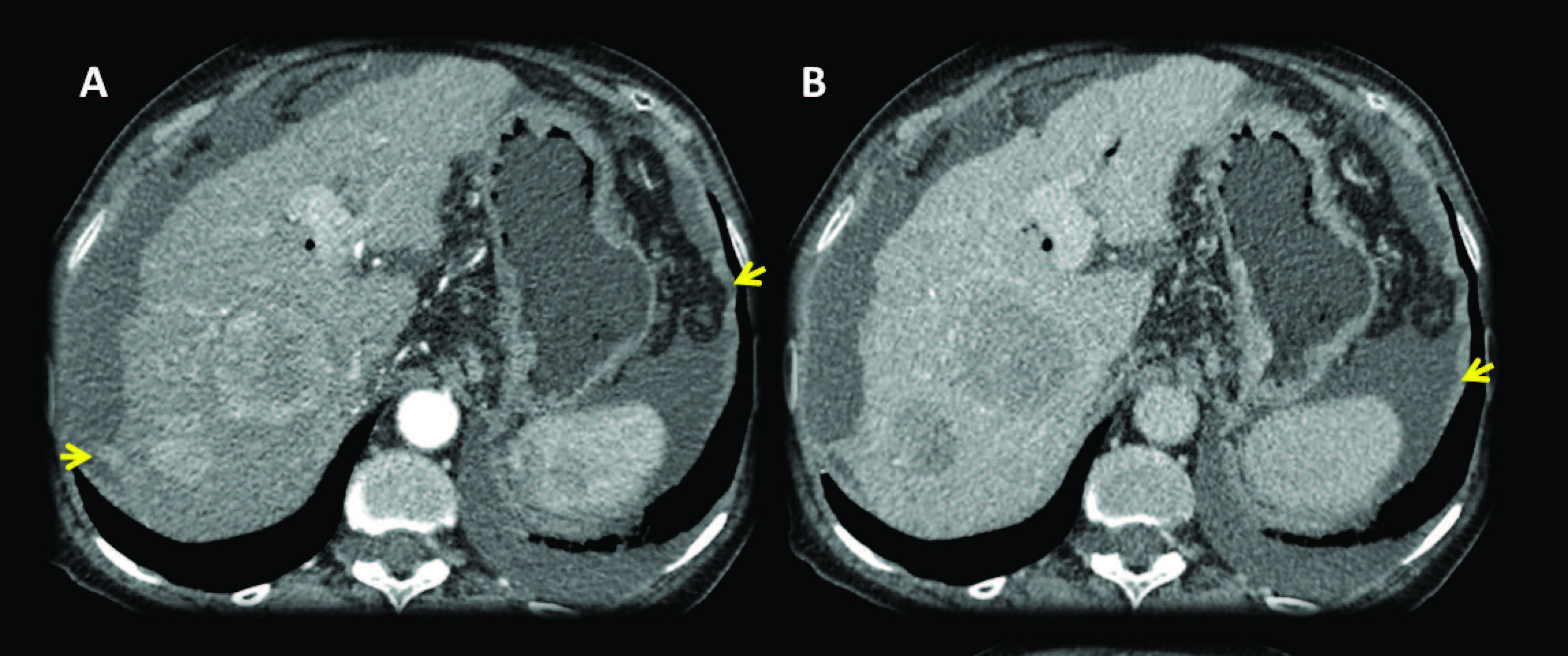
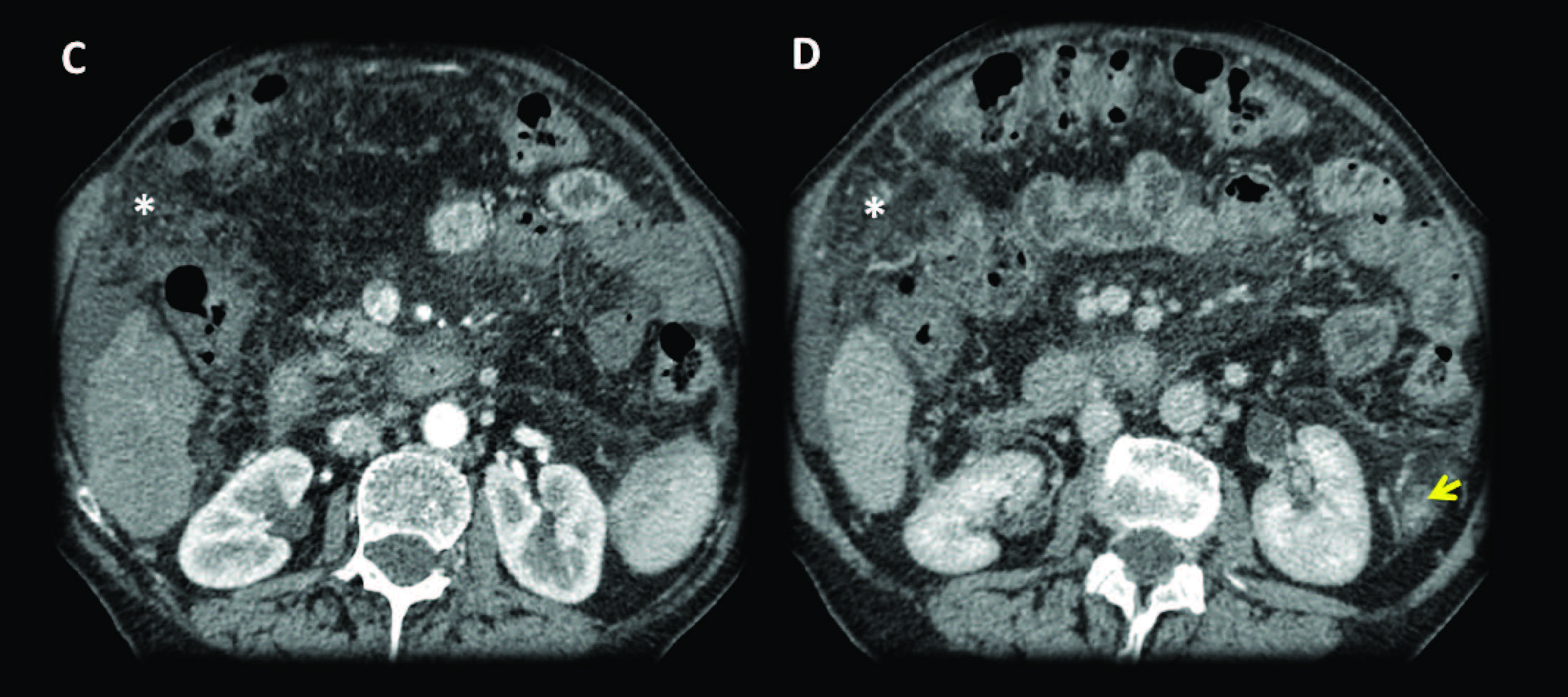
Figure 7.1. Mary Joseph Sister nodule (Images 7.1E, 7.1F). Very rare case of peritoneal and omental involvement in an advanced case of cirrhosis complicated with HCC.
Pathophysiology
The mechanism which these tumors spreads to the umbilicus remains unclear, however, several hypotheses has been developed including 3 possible dissemination pathways: contiguity, lymphatic and hematic spreading (Figure 6). The umbilicus is extensively connected to intraabdominal spaces due to several embryological remnants structures, and holds a considerable amount of vascular anastomotic structures and peritoneal ligaments as a convergence point.10
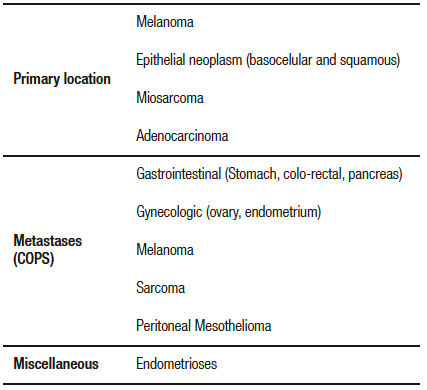
Despite 90% of the neoplastic lesions in the periumbilical area correspond to metastases; a not despicable 10% are primary malignancies of the local tissue being vitelline and uracus remnants adenocarcinomas the most frequent malignancies in this group (Table 1). Less than 1% of this nodule has benign nature like endometrium (Villar’s nodule), epithelial cysts and fibrotic tissue.
Figure 6. Illustrative scheme of the possible routes of dissemination of an advanced left colonic neoplasm. Transmural, omental, peritoneal and cutaneous periumbilical metastatic nodule (SMJN) involvement are represented. In this scheme the direct extension mechanism is characterized trough the mayor omentum.
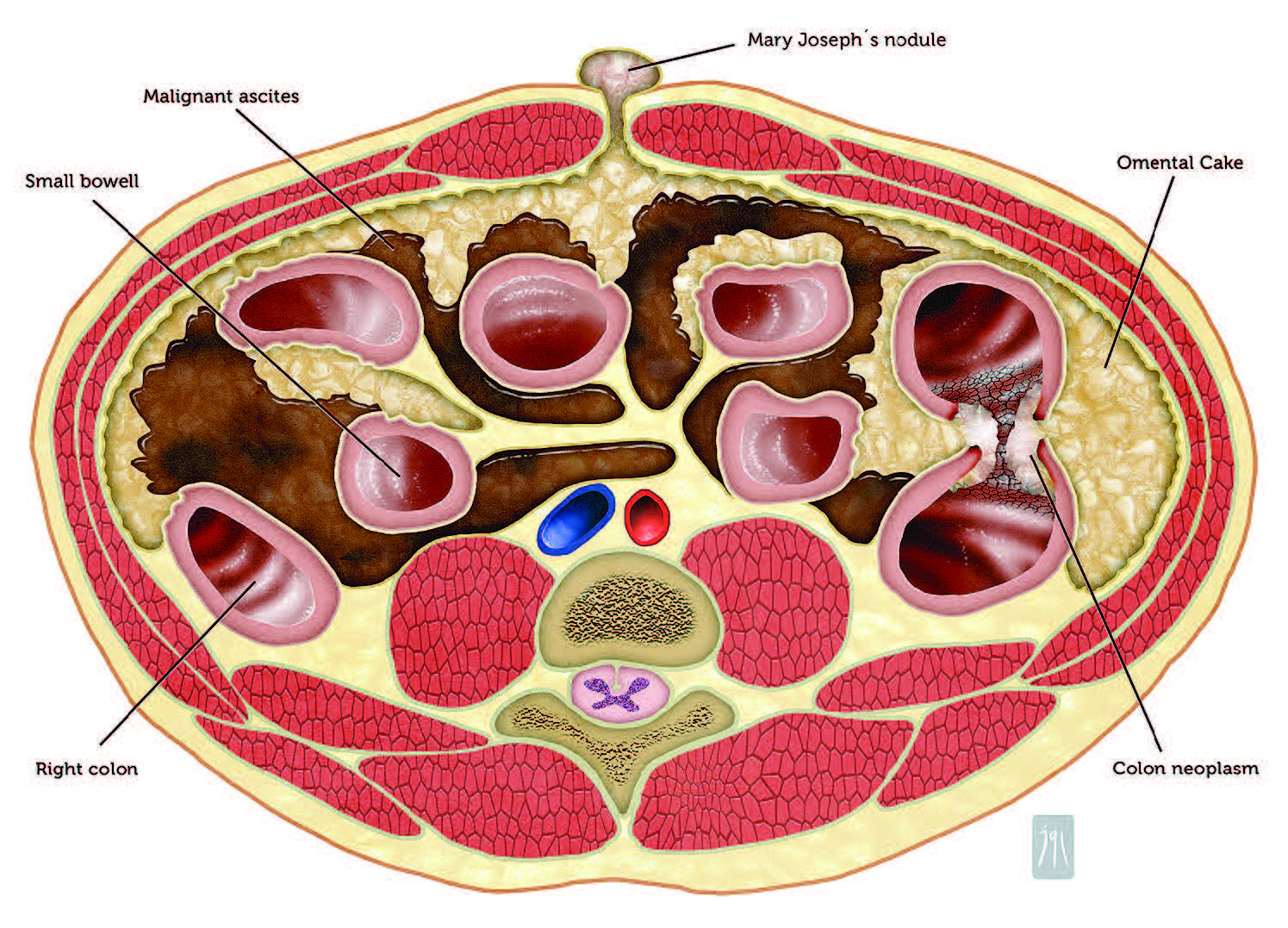
Table 1. Differential diagnosis of the cutaneous periumbilical nodules.
Imaging findings
SMJN, is usually found in patients between 40 and 70 years old (slightly more frequent in women) with history of weight loss and unspecific general symptoms and laboratory tests. In this context, a cancer of unknown primary is highly suspected. Imaging studies are essential to determine the origin of the primary neoplasm, and generally, at this point an advanced intraabdominal disease can be found.
Ultrasound images can help to clarify the clinical findings by detecting solid umbilical nodules, even if the diagnosis is difficult to make clinically. Thus, by itself the ultrasound images may not lead to the diagnose of the primary disease and usually require furthermore extensive examination.1
MDCT images allow the visualization of the cutaneous lesion and, in most of the cases; the primary lesion demonstrates its extension. Peritoneal or omental compromise like ascites and diffuse pseudo nodular involvement denotes a peritoneal carcinomatous process or omental cake.
A practical way to remember the main causes of the omental cake and the SMJN is using the acronym “COPS” that can be expanded as: colon, ovary, pancreas and stomach.11, 12
Discussion
The SMJN represents a cutaneous metastatic nodule located in the periumbilical cutaneous area. This nodule almost every time is a secondary location of an advanced intraabdominal malignancy and is considered as a very poor prognosis sign with an average life expectancy no greater than 6 months. Careful examination of all umbilical lesions is recommended. Most of the clinical diag-nosed SMJNs are metastases of intraabdominal carcinomas that are observables in MDCT studies; 52% of these cases are secondary locations of gastrointestinal neoplasms and a 28% are gynecologic metastases. Although the diagnose of the SMJN originally translated essentially an advanced cancer of unknown origin, today, its presence may represent up to 40%, recurrence of a previously treated malignancy.
The etiology of the primary malignancy determines the prognosis, and MDCT images and Fine Needle Aspiration Cytology of the tumor are invaluable in the diagnosis and recognition of the primary lesion.
The Sister Joseph`s nodule remains an interesting and valid useful radiologic and clinical sign in our days. Its correct diagnose is invaluable and the prognosis depends on it, radiologists must be aware.
Acknowledgements. Dr. Claudio Cortes for provide an extensive case collection and pictures and Julio García Lazo for the wonderful illustrations (contact: julio@ronins.cl).
Conflict of interest statement and founding. We declare that we did not have any conflict of interest at the submission time, and this paper did not receive any kind of external founding or sponsorship.
Referencias
- Gabriele R, Conte M, Egidi F, Borghese M. Umbilical metastases: current viewpoint. World J Surg Oncol 2005; 3: 13.
- Zhang K, Sankey C. The Sister Mary Joseph Nodule. J Gen Intern Med 2015; 30: 689-690.
- Trebing D, Göring HD. The umbilical metastasis. Sister Mary Joseph and her time. Hautarzt 2004; 55: 186-189.
- Dar IH, Kamili MA, Dar SH, Kuchaai FA. Sister Mary Joseph nodule – A case report with review of literature. J Res Med Sci 2009; 14: 385-387.
- Galvañ VG. Sister Mary Joseph’s nodule. Ann Intern Med 1998; 128: 410.
- Urbano FL, editor. Sister Joseph’s Nodule. Hosp Physician 2001; 37: 33-35.
- Dubreuil A, Dompmartin A, Barjot P, Louvet S, Leroy D. Umbilical metastasis or Sister Mary Joseph’s nodule. Int J Dermatol 1998; 37: 7-13.
- Gabriele R, Borghese M, Conte M, Basso L. Sister Mary Joseph’s Nodule as a First Sign of Cancer of the Cecum: Report of a Case. Dis Colon Rect 2004; 47: 115-117.
- Panaro F, Andorno E, Di Domenico S, Morelli N, Bottino G, Mondello R et al. Sister Joseph’s nodule in a liver transplant recipient: Case report and mini-review of literature. World J Surg Oncol 2005; 3: 4.
- Majmudar B, Wiskind AK, Croft BN, Dudley AG. The Sister (Mary) Joseph nodule: its significance in gynecology. Gynecol Oncol 1991; 40: 152-159.
- Al-Mashat F, Sibiany AM. Sister Mary Joseph’s nodule of the umbilicus: Is it always of gastric origin? A review of eight cases at different sites of origin. Indian J Cancer 2010; 47: 65-69.
- Touraud JP, Lentz N, Dutronc Y, Mercier E, Sagot P, Lambert D. Umbilical cutaneous metastasis (or Sister Mary Joseph’s nodule) disclosing an ovarian adenocarcinoma. Gynecol Obstet Fertil 2000; 28: 719-721.
Correspondencia: Ignacio Maldonado Schoijet
Av. Recoleta 464 (Zip: 8431657), Departamento de Imagenología,
Clínica Dávila. Santiago de Chile, Chile. Tel: +56 9 99641172
Correo electrónico: imschoijet@gmail.com
Acta Gastroenterol Latinoam 2018;48(2): 82-89