Karla P Aedo,1 Leslye F Conde,1 Reneé Pereyra-Elías1, 2
1 Escuela de Medicina, Universidad Peruana de Ciencias Aplicadas. Lima, Perú.
2 Policlínico de la Escuela de Oficiales de la Policía Nacional del Perú, Sanidad de la Policía Nacional del Perú. Lima, Perú.
Acta Gastroenterol Latinoam 2016;46:104-105
Recibido: 23/02/2016 / Aprobado: 04/04/2016 / Publicado en www.actagastro.org el 04/07/2016

Comunicación breve
Basada en el manuscrito original «Costo-efectividad de las pruebas de tamizaje del cáncer colorrectal en la Argentina», Acta Gastroenterol Latinoam 2016;46:8-17.
Ver EDITORIAL «Prevención del cáncer colorrectal»
Colorectal cancer (CCR) screening rates and success are very different among countries. This is unacceptable because of its highly preventable character. The natural history of this disease allows an advantage of an early detection and treatment of premalignant injuries.1 As an example, Australia implemented screening guidelines for CCR lowering mortality rates. As a consequence, patients with guidelines detected CRC got a markedly reduced risk of CRC recurrence and death compared to those cases with a clinical presentation.2
In 2013, the average mortality rate for CCR in South American countries was approximately 8,0%.3 However, this data is under estimated because of the lack of detection, the incorrect use of diagnostic exams and the fragmentation of the health systems mainly affecting primary care effectiveness.4
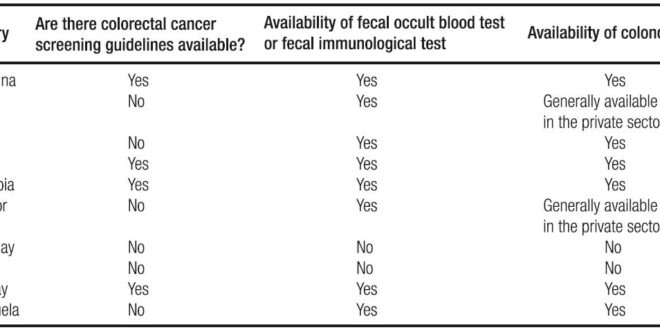
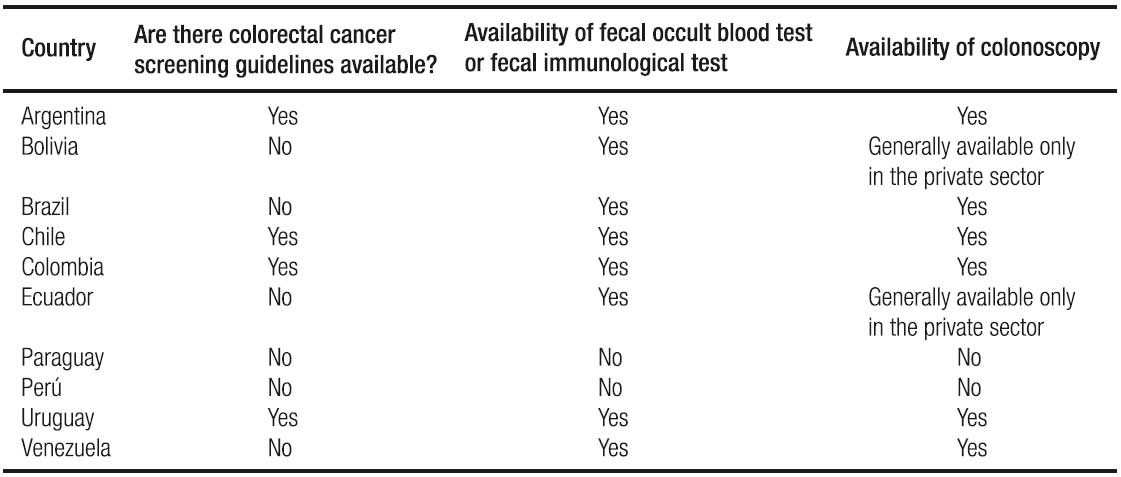
Despite the high mortality rate, a lot of South American countries do not have national practice guidelines for CCR screening (Table 1). Only four countries (Argentina, Chile, Colombia and Uruguay) have established formal recommendations. Four other countries have not guidelines, but screening instruments and exams are available for the population (public and private sectors). Finally, the situation in Peru and Paraguay is an emergency. These two countries do not have guidelines at all, and the availability of the screening exams is very limited.3
Tabla 1. Country profiles of colorectal cancer screening in South America.
Specifically, in Peru, the alert has been sent several times. Two years ago, Rebaza remarked the great importance of implementing this preventing service.5 Regard less of his recommendation, actually there was no change to this date. Also, we consider screening to be an initiative from all medical professionals at primary care specially general practitioners and not just from gastroenterologists or oncologists, which is the point of view of the afore mentioned author.5
Therefore, we reiterate the importance of the urgent implementation of integral and integrated programs of CCR screening in South American and other developing countries, which will bring an early detection and intervention.
Referencias
- Brenner H, Stock C, Hoffmeister M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014; 348: g2467.
- Ananda S, Wong H, Faragher I, Jones IT, Steele M, Kosmider S, et al. Survival impact of the Australian national bowel cancer screening program. Intern Med J 2015 [Epub ahead of print].
- Pan American Health Organization. Cancer in the Americas: Country Profiles 2013. Washington D C: PAHO; 2013.
- Ministerio de Salud. Análisis de la situación de cáncer en el Perú 2013. Lima: MINSA; 2013.
- Rebaza Vasquez S. Despistaje del cáncer colorrectal: ¿es necesario? Rev Gastroenterol Perú 2014; 34: 105-106.
Correspondencia: Leslye F Conde
Urb Alameda San marcos, Cda 2, Chorrillos. Lima, Perú
Correo electrónico: leslyecondeb@gmail.com
Acta Gastroenterol Latinoam 2016;46(2):104-105
